Dysarthria in children is a severe impairment of the pronunciation side of speech due to damage to the speech motor system.
Such a defect threatens the child with auditory perception disorder. The result is an inability to perceive information in full, problems with understanding the world around us, and maladjustment. In this case, great responsibility falls on the relatives of the little patient. Timely treatment will help restore the functioning of the speech organs, allow for correct pronunciation, and correction of all aspects of speech function.
Understand the problem
Nowadays, dysarthria is diagnosed in approximately 6% of children. This is a fairly high indicator to classify the disorder as common.
Despite the fact that the disease is quite common, many parents are confused when hearing the diagnosis of “dysarthria” in their child. Due to ignorance, treatment of a child’s pathology may be started late or follow the wrong plan. For children, it is important to do everything on time, including correcting pronunciation, otherwise the incorrect pronunciation model can be firmly fixed and remain forever.
With dysarthria, organic damage occurs to the facial muscles involved in the formation of speech: the muscles of the cheeks, tongue, and the area around the mouth. Nerve fibers innervating muscles and skin are also affected. As a result, facial expressions become impoverished. Dysarthric is deprived of the opportunity to fully work the facial muscles in order to pronounce the desired sound. The baby's speech becomes unintelligible, quiet, and monotonous.
Among the causes of the disorder are:
- severe toxicosis of pregnant women;
- Rhesus conflict;
- intrauterine infection;
- prematurity;
- premature birth;
- intrauterine fetal hypoxia;
- asphyxia of newborns;
- birth injuries;
- hereditary diseases;
- traumatic brain injury;
- hydrocephalus;
- infectious brain damage;
- intoxication of various origins;
- purulent otitis.
Dysarthria often accompanies cerebral palsy and mental retardation.
recognize their child’s illness at the beginning of their journey by the following signs:
- weakness of the facial muscles, accompanied by prolapse of the tongue, half-open mouth;
- spasm of the facial muscles - the child closes his lips tightly;
- late appearance of speech;
- problems with eating food – constant choking, difficulty swallowing, holding food in the cheek for a long time;
- increased salivation recorded after 6 months;
- the baby talks “in his nose” for no reason;
- speech without emotional coloring, too fast or slow. In case of increased tone of the vocal cords, the voice is squeaky;
- distortion, omission of individual sounds;
- impaired fine motor skills - difficulty fastening buttons or tying shoelaces. Cannot sculpt from plasticine, cannot draw due to weakness of holding a pencil;
- poor ear for music;
- speech breathing is impaired. Children, pronouncing a phrase, gasp, pause in pronunciation;
- complete muteness is possible due to paralysis of the facial muscles.
At 5 years old, the articulation of all sounds should be formed. If this does not happen, then the existing tongue-tiedness cannot be attributed to age. Specialist intervention is required. The sooner children go to a speech therapist, the better for them and their parents.
Often the problem is diagnosed as a rib at the age of about 7 years, before entering school. This age is considered late for the start of correction; the work will be more difficult and more effort will be required.
Causes of dysarthria
Dysarthria in children accompanies cerebral palsy in 65-85% of cases.
In less pronounced forms, it can appear in case of problems that arose during the prenatal period, the birth period, and even during the early development of the child. There are many causes of the disease during pregnancy and childbirth:
- serious toxicosis during pregnancy;
- Rhesus conflict;
- hypoxia;
- the presence of chronic somatic diseases in the mother;
- problems during childbirth - asphyxia, trauma, premature birth, pathologies during childbirth;
- kernicterus of newborns.
After birth, even if no pathologies have arisen in the nervous system in the womb or during childbirth, the risk of developing cerebral palsy still remains. Its appearance can be stimulated by neuroinfections, serious poisoning, trauma, purulent otitis media, and hydrocephalus.
Adults may also experience speech impairment if the brain has been damaged by disease, injury, or tumors. The development of a speech defect is provoked by:
- stroke;
- a brain tumor;
- multiple sclerosis;
- Parkinson's disease;
- myasthenia gravis;
- myotonia;
- neurosyphilis, etc.
Where to start treatment
Treatment of any disease must begin with a correct diagnosis. A young patient is first referred to a neurologist for consultation. After the examination, the specialist, if necessary, prescribes examinations :
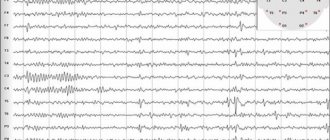
- EEG;
- electromyography;
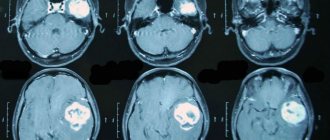
- MRI;
- electroneurography;
- transchannel magnetic stimulation.
After the diagnosis is established, the child is sent to a speech therapist who conducts special speech therapy tests. They allow you to determine the degree of the disease and its form. Subsequently, a neuropsychiatrist and a defectologist are involved in the process.
There are four degrees of the disease :
- 1st degree – the diagnosis is established only through special tests by a competent specialist;
- 2nd degree – speech is understandable, but has minor defects;
- 3rd degree – only close relatives understand the speech;
- 4th degree – speech is incomprehensible or absent.
Depending on the degree of the disorder, the specialist prescribes treatment and carries out corrective measures.
Classification
Neurologists and speech therapists are still actively discussing a generally accepted classification of dysarthria, but consensus has not yet been reached. The classification of dysarthria, which is based on the localization of the pathological focus, includes the following types:
- Bulbar dysarthria - associated with the involvement in the pathological process of the nuclei of the cranial nerves, which are localized in the medulla oblongata;
- Pseudobulbar dysarthria - in which the pathology concerns the pathways connecting the motor centers of the cortex with the nuclei of the bulbar nerves;
- Subcortical dysarthria - in which the subcortical nuclei of the brain are affected;
- Cerebellar dysarthria – pathology of the cerebellum and its pathways;
- Cortical dysarthria is a focal pathology of the cerebral cortex itself.
The classification of dysarthria according to the degree of severity divides it into erased, mild, moderate and severe dysarthria.
The Yusupov Hospital has been successfully treating patients with this type of pathology for many years. Doctors achieve tremendous results not only with erased dysarthria, but also with severe disease. Make an appointment
Sequence of treatment measures
If you believe that the treatment of dysarthria comes down to visits to a speech therapist, where the dysarthric person is taught to form a tube with his lips, then your opinion is wrong. There is a certain sequence of events, which is not recommended to be violated.
Elimination of dysarthria begins with restoration of the speech-motor system. To do this, the baby is given a speech therapy massage to develop fine motor skills. Breathing exercises are also used.
Speech therapy massage is one of the most effective methods of restoring the functioning of the speech apparatus. Massage affects the muscles, allowing them to normalize their tone. Therefore, the specialist first determines its level: hypo- or hypertonicity.
Speech therapy massage is divided into several types:
- manual;
- mechanical;
- hardware.
The manual technique is based on the impact of fingers on certain areas of the cheeks, lips, and tongue. The specialist carries out stroking and slight kneading of the muscle frame of the lips, cheeks and chin. Connects lips with fingers in vertical and horizontal positions. Massages the soft palate.
Mechanical technique involves influencing problem areas using special probes.
The hardware method uses vacuum, vibration, and temperature devices. It allows you to restore the nerve pathways connecting muscles with centers in the brain.
Dysarthric children are able to independently massage at home. simple exercises for this :
- baring teeth;
- lip stretching;
- open - close your mouth;
- the child puts a candy on a stick in his mouth, the adult takes it out. The smaller the volume of candy, the more difficult it is to do the exercise.
Massage allows you to:
- restore normal muscle tone;
- eliminate pathological movements of speech muscles;
- increase the amplitude of articulatory actions;
- makes muscles work that were not previously involved in the process;
- coordinates the movement of speech organs.
Breathing exercises
Speech
breathing is a complex process consisting of a strict relationship between the respiratory act and articulation. In small dysarthrics, such coordination is impaired. Before pronouncing the phrase, children take insufficient breath. They are able to speak while inhaling or at the very end of exhaling. Non-speech breathing is characterized by superficiality and rhythm instability.
Correct speech breathing ensures smoothness and softness of speech. With dysarthria, it is very important to improve this aspect of the process. Breathing exercises were developed for this purpose.
The most effective is breathing exercises according to A.N. Strelnikova . This is a set of original exercises that have no analogues in the world. The exercises focus on inhalation. It should be sharp, short, and delivered through the nose. When exhaling, attention is minimal. It is carried out arbitrarily.
There are main rules for performing exercises , if followed, the effect will be noticeable very quickly:
- The child takes a sharp, emotional, active breath through his nose. An analogy is drawn with the feeling of burning. At the same time, you can repeat: “Anxiety, it smells like burning,” and inhale the air, as if sniffing. Attention is concentrated on inhalation.
- Exhalation is done through the mouth. We explain to the baby that there is no need to hold back the air coming out. Let it come out spontaneously, without control.
- Inhale should be done as if inflating a car tire. Frequency – 60-70 breaths/minute. Pause – up to 3 seconds. In one lesson you need to perform 1000-2000 repetitions.
- The exercise should be done easily, without tension, without leading to a state of lack of air. Everything is within accessible limits.
The lesson begins with a warm-up, and only then can you move on to the main part.
Examples of exercises:
- half squat We bring one leg forward, the other behind. We squat shallowly, leaning on the front leg. While squatting, we take a short, rhythmic breath;
- holding your breath. We take a short breath while leaning forward. We hold our breath while counting to eight. We gradually increase the quantity.
Development of fine motor skills
It would seem, what is the connection between correct speech and finger movement? It turns out that the center of speech and finger motor skills are located nearby in the brain, stimulating each other’s work. The better developed fine motor skills, the better and faster the development of speech.
Digging a little from the topic, I would like to simultaneously explain to parents that movement in general helps strengthen neural connections that allow you to remember new information. A sedentary child is difficult to teach.
Developing motor activity of the fingers allows you to enrich your vocabulary and improve the phonemic aspect of speech. There are many options for developing fine motor skills: modeling from plasticine; working with paper (sheets can be crumpled, torn, pieces plucked off, folded in a certain sequence); designing crafts, creating applications, collages will also develop creative thinking.
Specialists use finger gymnastics, special attributes to stimulate motor activity of the finger in:
- Pinch your earlobe between your thumb and index finger. Walk along the edge of the ear with massage movements;
- spread your fingers wide. Clap your palms until all fingers touch;
- bend your fingers. Using massaging movements, move from the ear to the crown;
- A child ties knots on a rope. Then he runs them over with his fingers;
- the use of various balls - corrugated, with spikes, stuffed with balls. Squeezing/unsqueezing them with your hands;
- use of expanders;
- clothespins, computer keyboards, phones with buttons.
There are many devices, specialized and household, that allow you to work on the development of fine motor skills. A specialist will tell parents about possible options and explain how to conduct classes independently at home.
Pronunciation correction
After establishing the functioning of the articulatory apparatus and restoring muscle activity, the speech therapist proceeds to correcting incorrect pronunciation.
Typically, children exhibit the following pronunciation inaccuracies:
- omission of individual sounds, often “r”;
- replacing some sounds with others - “wak” instead of “rak”;
- interdental pronunciation, the so-called lisp;
- in isolation the sound is pronounced correctly. Problems appear when entering a word.
If such changes were noticed by parents, then speech therapy work should begin immediately, without waiting for 5 years.
Pronunciation correction requires an individual approach. The specialist determines which sounds are preserved and pronounced correctly. Work begins with sounds distorted to the least extent possible. Before performing them, it is necessary to teach children to distinguish them by ear.
The specialist’s task boils down to the following:
- modeling of basic articulation patterns - production of hissing, whistling, sonorant, palatal sounds;
- production of isolated sound;
- sound fixation, automatic inclusion in speech. First, for fixation, words are used in which the sound is present in an exaggerated form. Then any words with the desired sound symbol;
- pronunciation of a sound with an oppositional sound: sa-sha, sfa-tfa.
A speech therapist, in addition to the pronunciation aspect of speech, teaches the child lexical and grammatical basics, develops phrasal speech, and gives the basics of writing and reading skills.
Symptoms
Dysarthria is a deviation characterized by unclear, incomprehensible, slurred speech due to the fact that the muscles of the soft palate, tongue, larynx, vocal cords, and respiratory muscles function poorly. Defects in the presence of this disease are varied, and many of them overlap with other types of speech disorders, for example, there is a weak, quiet, muffled, nasal voice. Dysarthria is diagnosed based on the following symptoms:
- muscle hypotension;
- muscular dystonia;
- muscle spasticity;
- violations of sound pronunciation - erased dysarthria is characterized by blurred speech, more severe degrees - slow speech, slurring, omission of sounds, distortions, at 4 degrees - absence of speech.
Specific features that manifest dysarthria in children and adults are persistence of defects, learning difficulties, a longer period for automation, violation of both vowels and consonants, interdental and lateral pronunciation of sibilants and sibilants. Illness in children may be accompanied by OHP and dysgraphia.