General information
Meniere's disease and syndrome is one of the rare non-purulent diseases of the inner ear, which is caused by an increase in the volume of intralabyrinthine fluid and pressure, accompanied by attacks of dizziness , deafness, and balance disorders. It was first described by Meniere P., who noted that the pathology occurs in 0.02-0.2% of the population, more often in middle-aged Caucasians (30-50 years), but can also develop in children.
Meniere's syndrome: what kind of disease?
The pathology is vestibular neuronitis and is classified as idiopathic - developing independently, and not against the background of other ailments. Should be limited only to manifestations of peripheral labyrinthine syndrome without signs of central disharmonization or dissociation of pathological reactions.
The disease that most often causes recurrent systemic vestibular vertigo, tinnitus and sensorineural hearing loss .
Symptoms
Meniere's syndrome has a paroxysmal course. Suddenly there is an attack of dizziness, nausea and repeated vomiting, and noise appears in the ear. Patients complain that everything moves or rotates around them. They feel as if they are falling through, swinging or spinning on their own. “The world is turning upside down” - this is how patients describe their feelings at the time of an attack. Severe dizziness makes it difficult to sit or stand quietly. Patients are in a forced position. They usually lie down and close their eyes. Any movement brings suffering, nausea intensifies, vomiting occurs, which does not bring relief, and the general condition rapidly deteriorates.
Manifestations of the disease include:
- Congestion and tinnitus,
- Discoordination of movements,
- Loss of balance
- Hearing loss
- Hyperhidrosis,
- Dyspnea,
- Cardiopalmus,
- Pressure fluctuations,
- Pale skin
- Nystagmus,
- Forgetfulness,
- Short term memory loss
- Fatigue,
- Headache,
- Drowsiness,
- Depression,
- Visual impairment.
The attack lasts from 2 to 8 hours. It is usually preceded by an aura - increased tinnitus and slight loss of balance. An attack that occurs for no reason causes the patient to fall and be injured. Symptoms may persist after an attack. Patients feel weakness, weakness, fatigue, cephalalgia, and drowsiness. Symptoms of the pathology gradually intensify, hearing loss turns into deafness.
After the next attack or exacerbation, remission occurs, during which patients feel satisfactory. Efficiency is restored, the general condition is normalized. During the period of remission, heaviness and pain in the head, weakness, and general mild malaise may persist.
As the pathology progresses, attacks of dizziness become more frequent and severe. Patients lose their ability to work, cannot drive a car or engage in their favorite activities. They are always at home. The pathological process can pass from one ear to the other and lead to the development of complete deafness.
Pathogenesis
With Meniere's disease, there is an increase in the volume of endolymph inside the membranous labyrinth and, accordingly, an increase in pressure. As a result of such endolymphatic hydrops , caused by overproduction, disturbances of circulation and resorption of endolymph, patients experience:
- recurrent attacks of unilateral deafness that progress;
- signs of tinnitus;
- cases of systemic dizziness;
- disturbances in the sense of balance;
- autonomic disorders.
Most often, endolymphatic hydrops is asymptomatic, without progressing and without causing rupture of Reisner's membrane. It is the periodic ruptures of the membrane that cause the mixing of endolymph, rich in potassium, with perilymph, and as a result, depolarization and overexcitation of the vestibular nerve.
This leads to the development of paroxysmal dizziness. While hearing impairment and the occurrence of noise may be associated with the processes of apoptosis , death of spiral ganglion neurons, difficulty in conducting sound waves in the fluids of the labyrinth, and deterioration of the trophism of labyrinthine receptors.
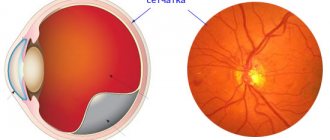
Inner ear of a healthy person and with Meniere's disease, expressed in an increase in the volume of endolymph
Important! When endolymphatic hydrops is secondary in nature, that is, the causes are directly related to another disease, then the concept of “Menière's syndrome” is distinguished.
Diagnostics
Diagnosing Meniere's disease can be difficult. The doctor cannot examine the inner ear directly, so there is no easy way to determine whether fluid has accumulated. Typically, a doctor will diagnose Meniere's disease if the person experiences typical symptoms and other possible causes of the symptoms have been ruled out.
The doctor will begin the diagnosis by taking a medical history, including information about past or current health problems and medications the patient has taken. He asks detailed questions about the symptoms, including when they started, how often and how long they last, and their severity. Then the doctor examines the ears, nose, and throat with special attention.
Tests that may be performed for diagnosis include:
- A hearing test, also called audiometry. This simple test can help you determine if you have a hearing problem. People with Meniere's disease have a certain type of nerve damage important to normal hearing, which can make it difficult to distinguish between similar-sounding words.
- Computed tomography (CT) or magnetic resonance imaging (MRI), scans that allow doctors to see the brain, middle ear, and other structures inside the head—scans can check for tumors and other problems that may cause symptoms similar to Meniere's syndrome.
- Electronystagmography or rotational testing - tests check the neural connection between the ears and eyes to examine the body's balance system. Electrodes are placed near the eyes in a darkened room. The ear canal is then stimulated with water, air or changes in position. Electrodes measure the response of the inner ear. In Meniere's disease, your doctor can identify typical changes caused by fluid buildup in the inner ear.
Classification
Depending on the development of the clinical picture, three variants of the course of Meniere’s disease are distinguished:
- the first (classic) type - there is a simultaneous development of vestibular and auditory disorders, that is, the first attack of vertigo leads to decreased hearing and tinnitus;
- the second - cochlear , is characterized by the appearance of initially auditory disorders, which are later joined by vestibular ones;
- the third most rare is vestibular , characterized by the presence at first only of attacks of dizziness, and hearing problems develop within a year after the debut of the pathology.
Treatment
Treatment of Meniere's disease is aimed at stopping and preventing the occurrence of attacks. Depending on the severity of the disease, treatment can be conservative or surgical. At the first symptoms, you should contact an otolaryngologist or neurologist.
Treatment for an attack of Meniere's disease
To relieve an attack of Meniere's disease, the patient is placed on a hard surface.
The eyes should be open and fixed at a fixed point, a heating pad may be applied to the legs, and exposure to loud sounds and bright lights should be removed. In order to relieve an attack of Meniere's disease, drugs are used that can relieve endolymphatic hydrops (diuretics), which leads to a decrease in intralabyrinth pressure. Symptomatic therapy is aimed at normalizing mental status, relieving vomiting and dizziness.
- During an attack, it is effective to administer atropine (subcutaneously 1 ml of 0.1% solution) to relieve impulses from the irritated labyrinth, 40% glucose solution;
- To eliminate this, dimenhydrate, a vestibular receptor blocker, is used. The effectiveness of betahistine has now been proven. The drug is able to cause dilation of the vessels of the inner ear, which leads to better blood supply, reabsorption and a decrease in the amount of endolymph. Papaverine is also sometimes used among vasodilators;
- In order to eliminate vomiting, antiemetic (antiemetics) drugs of central and peripheral action are used. The most popular substances are in release forms for intramuscular and rectal administration, since during an attack it is often impossible to take them orally due to profuse vomiting. These drugs include metoclopramide and thiethylperazine. Among the substances in the oral form are Bonin, Aviamarin, Ciel;
- To normalize the patient's mental state, sedatives are administered. Diazepam, Lorazepam, Mexidol have a pronounced anxiolytic effect;
- The use of diuretics in Meniere's disease is aimed at increasing diuresis, relieving ear congestion and, as a result, reducing the volume of endolymph (Manit, Diacarb). The use of diuretics must be combined with potassium supplements (Asparkam, Panangin).
A course of intravenous infusion of sodium bicarbonate will help normalize the alkaline reserve of the blood.
Causes
Scientists have not yet fully elucidated the etiology of Meniere's disease, but people with intellectual work and residents of large cities are more prone to the disease. The pathology may be caused by:
- vascular diseases;
- head or ear injuries;
- autoimmune, inflammatory or infectious processes in the inner ear;
- increased intracranial pressure ;
- hypertensive crisis;
- disruption of the functioning of the nerves innervating the vessels of the inner ear;
- congenital disorders, such as Mondini dysplasia .
Causes of Meniere's syndrome
The most common theory about the occurrence of the disease is a change in fluid pressure in the inner ear. The membranes located in the labyrinth gradually stretch as pressure increases, which leads to impaired coordination, hearing and other disorders.
The cause of increased pressure may be:
- Blockage of the drainage system of the lymphatic ducts (as a result of scarring after surgery or as a congenital malformation);
- Excessive fluid production;
- Pathological increase in the volume of pathways conducting fluid in the structures of the inner ear.
Anatomical enlargement of the inner ear is the most common condition diagnosed in children with unexplained sensorineural hearing loss. In addition to decreased hearing impairment, some patients experience coordination disorder, which can cause the development of Meniere's disease.
Since research has revealed that not all patients with Meniere's syndrome have increased fluid production in the labyrinth and cochlea, the immune status of the patient has become an additional factor causing the occurrence of the disease.
Increased activity of specific antibodies in the examined patients is detected in approximately 25% of cases. In the same amount, autoimmune thyroiditis is detected as a concomitant disease, which confirms the role of the immune status in the development of the disease.
According to the latest data, the causes of Meniere's disease in patients examined in 2014 remain unclear. Risk factors include:
- Viral diseases of the inner ear;
- Head injuries;
- Congenital abnormalities of the structure of the hearing organs;
- Allergies and other immune system disorders.
Symptoms of Meniere's disease
Manifestations of inner ear disease can begin with disturbances in the functioning of the vestibular apparatus, as well as with deterioration in hearing acuity, ear congestion and the occurrence of tinnitus. The first few years of hearing loss are transient, hearing fluctuations are observed, and between attacks an almost complete restoration of hearing levels can be observed. In the future, the signs of the syndrome only intensify and a gradual decrease in the level of hearing leads to its complete loss.
The main symptoms of Meniere's syndrome are:
- systemic attacks of dizziness lasting up to 20 minutes, which occur quite often with some regularity;
- imbalance, manifested in the inability to walk and maintain the body in a standing or even sitting position;
- flushes of nausea and vomiting;
- the occurrence of spontaneous nystagmus , but only during attacks;
- increased sweating ;
- changes in blood pressure, often downward, less often upward, which can be expressed in pallor of the skin;
- the occurrence of unpleasant sensations, ringing or noise ( tinnitus ) in one or both ears (occurs in no more than 15% of patients);
- feeling of ear fullness or deafness;
- ataxia;
- incoordination;
- reduced body temperature.
Among the permanent disorders are a progressive decrease in hearing and tinnitus . And if at first these manifestations are one-sided, then over time the pathology spreads to the second ear, causing complete deafness.
This labyrinthopathy is quite unpredictable, the symptoms vary in severity and intensity, causing the patient either a worsening of the condition, the addition of new manifestations, or, on the contrary, the disappearance of some defects. For example, labyrinthine attacks and dizziness can begin suddenly, vary in duration and frequency, which significantly reduces the quality of life and makes it incapacitating. A person is deprived of the opportunity to drive a car or operate other complex mechanisms, engage in various activities, go to work, and over time, for safety reasons, remains at home more and more often.
Peripheral labyrinthine syndrome is characterized by a phased course. During the period of exacerbation over several weeks, attacks of dizziness can occur quite often and be repeated several times, and vestibular manifestations do not disappear completely, but only subside. Then comes remission and a phase of well-being for months and even years. But as the disease progresses, the symptoms become more pronounced and even during remission the person experiences general weakness, mild imbalance and a feeling of heaviness in the head.
It is interesting that in some cases Meniere's syndrome went away on its own and did not recur, and many patients noticed that after 7-10 years the symptoms gradually decreased in severity and frequency - attacks of dizziness , tinnitus were less common or did not occur at all and hearing at the same time returned to normal.
Clinical picture
P. Meniere in his description of the wedge, the manifestations of the disease, named three main symptoms: hearing loss, noise in the ear (see Tinnitus) and paroxysmal dizziness (see), accompanied by balance disorders, nausea, vomiting, changes in cardiovascular activity, digestive, urinary systems, increased sweating (see Vestibular symptom complex). Simultaneous impairment of auditory and vestibular functions, i.e., the classic picture of M. b., occurs only in 35-46% of patients; in approximately half of the cases, the disease begins with auditory disorders and in 15-20% of cases with vestibular disorders. The time gap between auditory and vestibular (or between vestibular and auditory) disorders can be different - several days, weeks, months, years.
Hearing impairment in M. b. referred to as hearing loss in endolymphatic hydrops. For hearing loss (see) the following is characteristic. 1. Uniform increase in hearing thresholds over the entire frequency range with both air and bone sound conduction. 2. Predominantly low-frequency hearing loss in the early stages of the disease with preserved auditory sensitivity to ultrasound and normal ultrasonic stimulation thresholds in most patients. 3. Fluctuating hearing or fluctuating hearing loss (fluctuations in hearing acuity, pure tone threshold audiometry results, as well as tinnitus and ear congestion); tinnitus and ear congestion increase before an attack, often being its precursor, reach a maximum during an attack, and after it noticeably decrease, often accompanied by an improvement in hearing. 4. The positive phenomenon of accelerating the increase in volume (see Audiometry), detected very early and in almost 100% of observations. 5. Violation of clear speech perception, which usually concerns an increase in intelligibility thresholds; A small proportion of patients do not have 100% speech intelligibility.
The most severe symptom of M. b. are attacks of dizziness. Dizziness is most often manifested by a sensation of rotation or displacement of surrounding objects (visual), less often by a feeling of falling through, rotation of one’s own body (tactile). The severity of the patient's condition during an attack is largely determined by the severity of vegetative symptoms (nausea, vomiting, increased sweating, decreased blood pressure, decreased body temperature, increased urination). During an attack, spontaneous nystagmus is often observed (see), which is detected during visual observation in 65-70% of patients, with nystagmography (see Electronystagmography) - in more than 90%.
According to most researchers, the predominant type of dysfunction of the vestibular analyzer during experimental tests is hyporeflexia, indicating a decrease in the excitability of the receptors of the semicircular canals. In 12% of patients, a symptom of predominance of experimental nystagmus in direction is detected, in 2% - general hyperreflexia. It is assumed that with M. b. there may be a reversible and irreversible stage of endolymphatic hydrops. The reversible stage of hydrops (while the endolymphatic system can expand due to the perilymphatic system) is clinically characterized by typical attacks with light intervals, vestibular dysfunction during the period of remission is completely relieved, and impaired auditory function is manifested by fluctuating hearing loss with signs of more pronounced damage to the sound-conducting system of the inner ear. At the irreversible stage, attacks become very frequent and prolonged, light intervals almost completely disappear, hearing quickly and sharply deteriorates, acquiring the features of sensorineural hearing loss, spontaneous vestibular disorders are also detected in the interictal period. The stage of hydrops can also be judged by the glycerol test (ingestion of a mixture of glycerin half and half with water or fruit juice at the rate of 1 g of glycerin per 1 kg of body weight). A test is considered positive if the tonal hearing thresholds improve by no less than 10 dB and at no less than three frequencies, and the parameters of nystagmus reactions during vestibular tests change by no less than 25% relative to the initial values.
A positive glycerol test indicates the reversibility of hydrops.
Tests and diagnosis of Meniere's disease
To identify idiopathic endolymphatic hydrops underlying Meniere's disease, a comprehensive assessment of the results of a number of tuning fork studies, threshold audiometry, auditory sensitivity, as well as taking into account medical history, collecting patient complaints and clinical manifestations of the disease is necessary.
Diagnostics includes electrocochleography, pure tone threshold audiometry, ultrasound tests, a test to determine the lateralization of loud sounds, dehydration test, extratympanic electrocochleography, otoacoustic emission, and functional computer stabilography.
Procedures and operations
For patients suffering from Meniere's disease or syndrome, gentle surgical interventions may be recommended:
- drainage of the endolymphatic sac - helps reduce pressure in the endolymphatic area and reduce the severity of symptoms without harming the structures of the affected ear;
- sacculotomy is a decompressive surgical intervention, which is an opening of the membranous spherical sac of the vestibule of the ear labyrinth;
- intersection of the vestibular-vestibular nerve eliminates afferent impulses and relieves vestibular disorders;
- laser destruction carried out on the horizontal semicircular canal allows patients to get rid of attacks of dizziness, delay the development of hearing loss and disorders in the second ear.
In extreme cases, they resort to decompressive and destructive operations ( labyrinthectomy, cochleosacculotomy, vestibular neurectomy , etc.), because they can lead to one-sided deafness and resumption of attacks of sensorineural dizziness.
Treatment of Meniere's disease with folk remedies
Despite the fact that the disease is incurable, many do not want to give up or take medications for the rest of their lives; in such cases, medicinal plants come to their aid. There are different ways to treat Meniere's disease with folk remedies:
- sunflower root - its decoction can help; the root, collected in the fall, needs to be crushed and a glass of the raw material boiled in 3 liters of water for 2 hours, it should be drunk no more than 2 days before, the course is long - a month or more;
- black radish - juice is also used, which is recommended to drink 1 teaspoon. spoon after meals, and cakes - they need to be mixed with honey and eaten 2 tablespoons. spoons 3 times a day;
- birch leaves and horsetail grass - you need to prepare a decoction, taking 30 g of raw material per glass of water, cook for no more than 5 minutes, drink this glass of decoction throughout the day;
- nettle root - can be brewed as tea, 2 teaspoons is enough. spoons of vegetable raw materials;
- ash after burning bean stalks - it needs to be ground into powder and mixed 0.5 teaspoon. spoons from 1 table. spoon of vodka, take 3 times a day.
Diet for Meniere's disease
Salt-free diet
- Efficiency: 5-10 kg in 13 days
- Time frame: 13 days
- Cost of products: 4500-8000 rubles for 13 days
In addition to drug therapy, non-drug treatment methods play a fairly important role in the prevention and relief of attacks caused by pathology, one of which is following a special diet. She bans some foods and drinks and makes recommendations for creating a daily menu. It is strictly prohibited for people suffering from Meniere's disease to:
- too salty foods, including store-bought snacks (crackers, nuts, chips), canned and soaked vegetables, and there should also be a strict limit on the consumption of table salt - no more than 1-1.5 g per day;
- alcohol and caffeinated drinks.