Brain tissue is represented by a wide range of formations. In terms of its structure, it is perhaps the most complex part of the human body, which determines the wide nature of the activity of the central nervous system. When assessing the structure, several areas of the central nervous system can be identified in this localization.
At the base of the cerebral structures is the so-called brain stem. It provides a group of vital functions: from breathing and cardiac activity to thermoregulation. Any damage or malfunction results in severe disability or death.
The pons is a component of the brainstem located between the midbrain and medulla oblongata, which ensures normal conduction of nerve impulses and makes it possible to perform a number of voluntary actions.
Responsible for some functions of higher activity. Its damage, for example, due to injury or stroke, leads to critical disruptions in the functioning of the entire body.
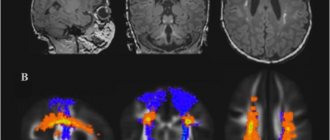
Diagnosis of lesions of this anatomical structure presents certain difficulties due to the deep and “inconvenient” localization. The only reliable method of examination is MRI or, less commonly, computed tomography.
Structure
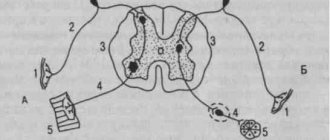
The pons is located at the level of the brain stem and two main areas are conventionally distinguished in its anatomy.
- Top part. It consists of gray matter and includes several pairs of cranial nerves (from the 5th to the 8th). This is the actual functional structure.
- The lower or base - ensures the conduction of signals, acts as a transport route for natural impulses.
At the level of the upper part of the bridge there is a reticular formation. It is represented by a large accumulation of fibers that allow the entire central nervous system to function in a harmonious manner.
At the base there is a dense layer of thick conductive strands. They are three legs on each side, connected to the cerebellum and enable the extrapyramidal system to work.
Below the pons is the medulla oblongata, in the upper part is the middle brain.
There are some differences in the structure of this education in children and adults. When evaluated in patients under 8 years of age, a complete absence of the myelin sheath is found, which is considered normal.
The development of this part of the brain is observed in early adolescence. The anatomy of the bridge is complex, which is explained by the need to carry out a number of actions on the part of the central nervous system.
Parts of the brain and their functions: cortex
The cortex controls several specific functions of the body. Each share is responsible for its own parameters. Let's take a closer look at the functions associated with calving:
- temporal – controls the sense of smell and hearing;
- parietal – responsible for taste and touch;
- occipital – vision;
- frontal – complex thinking, movement and speech.
Each neuron contacts other neurons, there are up to ten thousand contacts (gray matter). Nerve fibers are white matter. A certain part unites the hemispheres of the brain. White matter includes three types of fibers:
- association ones connect different cortical areas in one hemisphere;
- commissural connect the hemispheres to each other;
- projection ones communicate with lower formations and have analyzer paths.
Considering the structure and functions of parts of the brain, it is necessary to emphasize the role of gray and white matter. The hemispheres inside have basal ganglia (gray matter), their main function is the transmission of information. White matter is located between the cerebral cortex and the basal ganglia. There are four parts here:
- between the grooves in the gyri;
- in the outer places of the hemispheres;
- included in the inner capsule;
- located in the corpus callosum.
The white matter located here is formed by nerve fibers and connects the gyral cortex with the underlying sections. The subcortical nuclei form the subcortex of the brain.
The telencephalon controls all the vital functions of the body, as well as the intellectual abilities of a person.
What functions does the bridge perform?
The pons is responsible for several important forms of activity.
Among them:
- Reflexive automatic and voluntary movements of the eyes and eardrum in response to loud sounds, as well as tissues of the oral cavity (palate). Any violation ends in problems.
- The ability for purposeful motor activity. Since the pons in the brain ensures the functioning of the cerebellum, any damage causes problems with the ability to control the body.
- Perception of vestibular stimuli. In this case, we are talking about the ability to perceive one’s body as a whole, its orientation and location in space, to respond to any changes in environmental conditions, and also to dampen unnecessary movements (for example, during sudden braking in public transport, stumbling, etc.). When affected, there is a lack of coordination. Ability to navigate in space.
- Providing olfactory function. The bridge has this ability partially. Other subcortical clusters are also responsible for it.
- Normal innervation of the skin and mucous membranes of the face.
- The pons is involved in the formation of sleep. This is a complex and coordinated work of several cerebral formations at once. Any violations immediately lead to problems with night rest. The patient becomes lethargic, asthenic processes appear.
- The functions of the pons include the acts of chewing and swallowing. Vital for nutrition and breathing.
- In fact, the body’s ability to perform normal gas exchange depends on the functioning of this structure. In the absence of adequate conduction of impulses, problems begin, even lethal disorders.
Basic actions are performed by nervous tissues constantly. Even minor changes are noticeable immediately.
The pons is part of the brain stem, therefore deviations in its activity become an indirect cause of dysfunction of this entire formation.
Complications, including rapid and fatal ones, are likely. High-quality medical care is not always possible due to the complex localization of structures and complex structure.
Medulla oblongata and pons, their participation in the processes of self-regulation of functions
The medulla oblongata in humans is about 25 mm long. It is a continuation of SM. Unlike the SM, it does not have a metameric, repeatable structure; the gray matter in it is not located in the center, but with its nuclei towards the periphery.
In the medulla oblongata there are olives associated with the SC, the extrapyramidal system and the cerebellum - these are the thin and wedge-shaped nuclei of proprioceptive sensitivity (Gaull and Burdach nuclei). Here are the intersections of the descending pyramidal tracts and the ascending tracts formed by the thin and wedge-shaped fascicles (Gaull and Burdach), the reticular formation.
The medulla oblongata, due to its nuclear formations and reticular formation, is involved in the implementation of vegetative, somatic, gustatory, auditory, and vestibular reflexes. A feature of the medulla oblongata is that its nuclei, being excited sequentially, ensure the execution of complex reflexes that require the sequential activation of different muscle groups, which is observed, for example, when swallowing.
The medulla oblongata contains the nuclei of the following cranial nerves:
• pair of VIII cranial nerves - the vestibulocochlear nerve consists of the cochlear and vestibular parts. The cochlear nucleus lies in the medulla oblongata;
• pair IX - glossopharyngeal nerve; its core is formed by 3 parts - motor, sensitive and vegetative. The motor part is involved in the innervation of the muscles of the pharynx and oral cavity, the sensitive part receives information from the taste receptors of the posterior third of the tongue; autonomic innervates the salivary glands;
• pair X - the vagus nerve has 3 nuclei: the autonomic innervates the larynx, esophagus, heart, stomach, intestines, digestive glands; the sensitive receives information from the receptors of the alveoli of the lungs and other internal organs, and the motor (the so-called mutual) ensures the sequence of contractions of the muscles of the pharynx and larynx during swallowing;
• pair XI - accessory nerve; its nucleus is partially located in the medulla oblongata;
• pair XII - the hypoglossal nerve is the motor nerve of the tongue, its core is mostly located in the medulla oblongata.
Sensory functions. The medulla oblongata regulates a number of sensory functions: reception of skin sensitivity of the face - in the sensory nucleus of the trigeminal nerve; primary analysis of taste reception - in the nucleus of the glossopharyngeal nerve; reception of auditory stimuli - in the nucleus of the cochlear nerve; reception of vestibular stimuli - in the superior vestibular nucleus. In the postero-superior parts of the medulla oblongata there are pathways of cutaneous, deep, visceral sensitivity, some of which are switched here to the second neuron (gracilis and cuneate nuclei). At the level of the medulla oblongata, the listed sensory functions implement a primary analysis of the strength and quality of irritation, then the processed information is transmitted to the subcortical structures to determine the biological significance of this irritation.
Conductor functions. All ascending and descending tracts of the spinal cord pass through the medulla oblongata: spinothalamic, corticospinal, rubrospinal. It originates the vestibulospinal, olivospinal and reticulospinal tracts, which provide tone and coordination of muscle reactions. In the medulla oblongata, the tracts from the cerebral cortex end - the corticoreticular tracts. Here the ascending pathways of proprioceptive sensitivity from the spinal cord end: the thin and wedge-shaped. Brain formations such as the pons, midbrain, cerebellum, thalamus, hypothalamus and cerebral cortex have bilateral connections with the medulla oblongata. The presence of these connections indicates the participation of the medulla oblongata in the regulation of skeletal muscle tone, autonomic and higher integrative functions, and analysis of sensory stimulation.
Reflex functions. Numerous reflexes of the medulla oblongata are divided into vital and non-vital, but this idea is quite arbitrary. The respiratory and vasomotor centers of the medulla oblongata can be classified as vital centers, since a number of cardiac and respiratory reflexes are closed in them.
The medulla oblongata organizes and implements a number of protective reflexes
: vomiting, sneezing, coughing, lacrimation, closing eyelids. These reflexes are realized due to the fact that information about the irritation of the receptors of the mucous membrane of the eye, oral cavity, larynx, nasopharynx through the sensitive branches of the trigeminal and glossopharyngeal nerves enters the nuclei of the medulla oblongata, from here comes the command to the motor nuclei of the trigeminal, vagus, facial, glossopharyngeal, accessory or hypoglossal nerves, as a result, one or another protective reflex is realized. In the same way, due to the sequential activation of the muscle groups of the head, neck, chest and diaphragm, reflexes of eating behavior are organized: sucking, chewing, swallowing.
In addition, the medulla oblongata organizes reflexes to maintain posture
. These reflexes are formed due to afferentation from the receptors of the vestibule of the cochlea and the semicircular canals to the superior vestibular nucleus; from here, processed information assessing the need to change posture is sent to the lateral and medial vestibular nuclei. These nuclei are involved in determining which muscle systems and segments of the spinal cord should take part in changing posture, therefore, from the neurons of the medial and lateral nuclei along the vestibulospinal tract, the signal arrives to the anterior horns of the corresponding segments of the spinal cord innervating the muscles that are involved in changing posture at a given time. moment is necessary.
Changes in posture are carried out due to static and statokinetic reflexes. Static
reflexes regulate the tone of skeletal muscles in order to maintain a certain body position.
Statokinetic
reflexes of the medulla oblongata provide redistribution of the tone of the trunk muscles to organize a posture corresponding to the moment of linear or rotational movement.
Most of the autonomic reflexes of the medulla oblongata are realized through the nuclei of the vagus nerve
, which receive information about the state of activity of the heart, blood vessels, digestive tract, lungs, digestive glands, etc. In response to this information, the nuclei organize the motor and secretory reactions of these organs.
Excitation of the vagus nerve nuclei causes increased contraction of the smooth muscles of the stomach, intestines, and gallbladder and at the same time relaxation of the sphincters of these organs. At the same time, the work of the heart slows down and weakens, and the lumen of the bronchi narrows.
The activity of the vagus nerve nuclei is also manifested in increased secretion of the bronchial, gastric, intestinal glands, and in the stimulation of the pancreas and secretory cells of the liver.
The center of salivation is located in the medulla oblongata
, the parasympathetic part of which ensures increased general secretion, and the sympathetic part - protein secretion of the salivary glands.
The respiratory and vasomotor centers are located in the structure of the reticular formation of the medulla oblongata. The peculiarity of these centers is that their neurons are capable of being excited reflexively and under the influence of chemical stimuli.
Respiratory center
localized in the medial part of the reticular formation of each symmetrical half of the medulla oblongata and is divided into two parts, inhalation and exhalation.
Another vital center is represented in the reticular formation of the medulla oblongata - the vasomotor center
(regulation of vascular tone). It functions together with the overlying structures of the brain and, above all, with the hypothalamus. Excitation of the vasomotor center always changes the rhythm of breathing, the tone of the bronchi, intestinal muscles, bladder, ciliary muscle, etc. This is due to the fact that the reticular formation of the medulla oblongata has synaptic connections with the hypothalamus and other centers.
In the middle sections of the reticular formation there are neurons that form the reticulospinal tract, which has an inhibitory effect on the motor neurons of the spinal cord. At the bottom of the fourth ventricle are the neurons of the locus coeruleus. Their mediator is norepinephrine. These neurons cause activation of the reticulospinal tract during REM sleep, which leads to inhibition of spinal reflexes and decreased muscle tone.
Symptoms of damage. Damage to the left or right half of the medulla oblongata above the intersection of the ascending pathways of proprioceptive sensitivity causes disturbances in the sensitivity and functioning of the muscles of the face and head on the side of the damage. At the same time, on the opposite side to the side of the injury, disorders of skin sensitivity and motor paralysis of the trunk and limbs are observed. This is explained by the fact that the ascending and descending pathways from and to the SC intersect, and the nuclei of the cranial nerves innervate their half of the head, i.e., the cranial nerves do not intersect.
The pons is located above the medulla oblongata and performs sensory, conductive, motor, and integrative reflex functions.
The bridge includes the nuclei of the facial, trigeminal, abducens, vestibular and cochlear nerves (vestibular and cochlear nuclei), the nuclei of the vestibular part of the vestibular nerve (vestibular nerve): lateral (Deiters) and superior (Bekhterev). The reticular formation of the pons is closely related to the reticular formation of the midbrain and medulla oblongata.
An important structure of the pons is the middle cerebellar peduncle. It is this that provides functional compensatory and morphological connections between the cerebral cortex and the cerebellar hemispheres.
The sensory functions of the bridge are provided by the nuclei of the vestibulocochlear and trigeminal nerves. The cochlear part of the vestibulocochlear nerve ends in the brain in the cochlear nuclei; the vestibular part of the vestibulocochlear nerve - in the triangular nucleus, Deiters nucleus, Bechterew's nucleus. Here the primary analysis of vestibular irritations of their strength and direction takes place.
The sensory nucleus of the trigeminal nerve receives signals from receptors on the skin of the face, the anterior parts of the scalp, the mucous membrane of the nose and mouth, teeth and the conjunctiva of the eyeball. The facial nerve innervates all facial muscles. The abducens nerve innervates the rectus lateralis muscle, which abducts the eyeball outward.
The motor portion of the trigeminal nerve nucleus innervates the masticatory muscles, the tensor tympani muscle, and the tensor palatine muscle.
Conductive function of the bridge. Provided with longitudinally and transversely located fibers. Transversely located fibers form the upper and lower layers, and between them there are pyramidal tracts coming from the cerebral cortex. Between the transverse fibers are located neural clusters - the nuclei of the bridge. From their neurons, transverse fibers begin, which go to the opposite side of the pons, forming the middle cerebellar peduncle and ending in its cortex.
In the tegmentum of the bridge there are longitudinally running bundles of fibers of the medial loop. They are intersected by transversely running fibers of the trapezoid body, which are axons of the cochlear part of the vestibulocochlear nerve of the opposite side, which end in the nucleus of the superior olive. From this nucleus there are pathways of the lateral lemniscus, which go to the posterior quadrigemina of the midbrain and to the medial geniculate body of the diencephalon.
The anterior and posterior nuclei of the trapezoid body and lateral lemniscus are localized in the tegmentum of the brain. These nuclei, together with the superior olive, provide the primary analysis of information from the organ of hearing and then transmit information to the posterior tubercles of the quadrigeminals.
The tegmentum also contains the long medial and tectospinal tracts.
The intrinsic neurons of the pons structure form its reticular formation, the nuclei of the facial, abducens nerves, the motor portion of the nucleus and the middle sensory nucleus of the trigeminal nerve.
The reticular formation of the pons is a continuation of the reticular formation of the medulla oblongata and the beginning of the same midbrain system. The axons of the neurons of the reticular formation of the bridge go to the cerebellum, to the spinal cord (reticulospinal tract). The latter activate spinal cord neurons.
The reticular formation of the pons affects the cerebral cortex, causing it to awaken or sleep. In the reticular formation of the bridge there are two groups of nuclei that belong to the common respiratory center. One center activates the inhalation center of the medulla oblongata, the other activates the exhalation center. Neurons of the respiratory center located in the pons adapt the work of the respiratory cells of the medulla oblongata in accordance with the changing state of the body.
Pathologies that impair the functions of the bridge and their symptoms
There is a group of diseases that are typically characterized by disruption of the normal functioning of the body as a result of the destruction of the tissues in question.
Among them:
Brissot-Sicard syndrome
Accompanied by a disorder of cranial nerve activity. It is determined by unilateral paresis or complete paralysis of half the body.
The ability to control the muscles of the facial area is also lost, and ptosis (drooping of the eyelid) with impaired visual function is possible.
This disorder occurs against the background of an infectious, autoimmune or tumor lesion. Less commonly, it results from cerebral ischemia. After a transient attack or a full-fledged stroke.
Bonnier syndrome
Characterized by damage to a group of cranial nerves. In this case, the auditory and vestibular nuclei ultimately suffer.
Symptoms are nonspecific. Problems arise with the perception of sound stimuli. Patients constantly experience dizziness, nausea, and weakness.
Insomnia is also part of the clinic. The patient becomes irritable, and emotional instability is noted. Up to sudden changes in phases, as, for example, with bipolar affective psychosis.
Grenet's syndrome
A typical feature of this pathological process is a violation of the sensitivity of facial muscles, which ultimately leads to problems with the manifestation of non-verbal signals and emotions.
There is partial paresis of the masticatory muscles on one side. On the other hand, controllability impairment is also present, but to a much lesser extent.
Ventral syndrome
An extremely difficult condition. It is characterized by at least loss of speech function. This is the easiest case.
The classic situation is determined by the complete loss of the ability to move. The man cannot move. Communication is possible only through the eyes.
This disorder persists for a long time. Quickly leads to stagnation and death of the patient. Restoration is not possible.
Raymond-Sestan syndrome
Characterized by a key manifestation of the oculomotor nerves. A person loses the ability to voluntarily focus his gaze and move it from one object to another.
Spontaneous relief of the condition and its subsequent return for unclear reasons is possible.
Hübler's syndrome
There are no specific manifestations of blood paralysis of facial muscles. The facial expression is characterized as a mask.
The patient is unable to adequately non-verbally express emotions and respond to surrounding stimuli.
Skin sensitivity also decreases, which is detected by the results of functional tests and physical examination.
Foville syndrome
There is paralysis of facial muscles and strabismus with visual impairment.
Gasperini disease
Combined pathological process. Characterized by mixed symptoms.
Diseases leading to the development of syndromes
The structure of the Varoliev bridge suggests many possible lesions and an equally large number of manifestations. However, there is a group of diseases that become the foundation for the above syndromes.
This may include:
- Stroke. Acute disruption of cerebral blood flow in one area or another with death of nerve tissue and loss of some functions of cerebral structures. If the brain stem itself suffers, in the most favorable case it will end in a violation of higher activity.
- Ischemic transient attacks. Incorrectly called microstrokes. The same thing is observed, but there is no significant tissue death.
- Atherosclerosis of cerebral vessels. Impaired arterial patency as a result of blockage of the arteries by cholesterol plaques or spontaneous narrowing due to, for example, long-term smoking, hypertension (increased pressure).
- Infectious processes. Especially those that affect cerebral tissue. Encephalitis, meningitis.
- Demyelination. Multiple sclerosis.
The Varoliev bridge is responsible for a lot of important functions and has a systematic structure. Treatment of pathological conditions when the activity of this structure is already impaired is an extremely complex and sometimes impossible process.
Therefore, it makes sense to have a preventive effect on all diseases that may become a source of problems in the future. This is an important preventative measure.