Secondary zones
In another way, these zones are called peripheral.
This name was not given to them by chance. They are located in the peripheral parts of the cortex. Secondary zones differ from the central (primary) zones in their neural organization, physiological manifestations and architectural features. Let's try to figure out what effects occur if the secondary zones are affected by an electrical stimulus or if they are damaged. The effects that arise mainly concern the most complex types of processes in the psyche. In the event that damage occurs to the secondary zones, the elementary sensations remain relatively intact. Basically, there are disturbances in the ability to correctly reflect mutual relationships and entire complexes of elements that make up the various objects that we perceive. For example, if the secondary zones of the visual and auditory cortex are damaged, then the emergence of auditory and visual hallucinations can be observed, which unfold in a certain temporal and spatial sequence.
Secondary areas are of significant importance in the implementation of mutual connections between stimuli, which are allocated with the help of primary areas of the cortex. In addition, they play a significant role in the integration of functions that are carried out by the nuclear fields of different analyzers as a result of combining into complex complexes of receptions
Thus, secondary zones are of particular importance for the implementation of mental processes in more complex forms that require coordination and which are associated with a detailed analysis of the relationships between objective stimuli. During this process, specific connections are established, which are called associative connections.
Afferent impulses entering the cortex from receptors of various external sensory organs reach secondary fields through many additional switches in the association nucleus of the thalamus, which is also called the thalamus optic. Afferent impulses going to the primary zones, in contrast to impulses going to the secondary zones, reach them via a shorter route. It is implemented through a relay core in the visual thalamus.
We figured out what the cerebral cortex is responsible for.
Anatomy and physiology of the cerebral cortex.
Cerebral cortex
or
cerebral cortex
(lat.
cortex cerebri
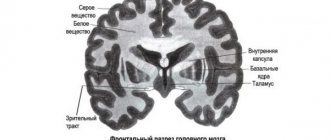
) - a structure of the brain, a layer of gray matter 1.3-4.5 mm thick, located along the periphery of the cerebral hemispheres and covering them. The greatest thickness is observed in the upper parts of the precentral, postcentral gyri and paracentral lobule.
The cerebral cortex covers the surface of the hemispheres and forms a large number of grooves of varying depth and length. Between the grooves there are cerebral convolutions of varying sizes.
In each hemisphere the following surfaces are distinguished:
1. convex superolateral surface adjacent to the inner surface of the bones of the cranial vault
2. the lower surface, the anterior and middle sections of which are located on the inner surface of the base of the skull, in the region of the anterior and middle cranial fossae, and the posterior ones - on the tentorium of the cerebellum
3. medial surface directed to the longitudinal fissure of the brain.
These three surfaces of each hemisphere, passing one into another, form three edges. The superior edge separates the superolateral and medial surfaces. The inferolateral edge separates the superolateral surface from the inferior one. The inferomedial edge is located between the inferior and medial surfaces.
In each hemisphere, the most prominent places are distinguished: in front - the frontal pole, in the back - occipital, and on the side - temporal.
Attention!
If you need help writing a paper, we recommend turning to professionals. More than 70,000 authors are ready to help you right now. Free adjustments and improvements. Find out the cost of your work.
Cost calculationGuaranteesReviews
The hemisphere is divided into five lobes. Four of them are adjacent to the corresponding bones of the cranial vault: 1 frontal lobe, 2 parietal lobe, 3 occipital lobe, 4 temporal lobe
The fifth, the insular lobe, is located deep in the lateral fossa of the cerebrum, separating the frontal lobe from the temporal lobe.
cortex has a five- or six-layer structure. Neurons
represented by sensory, motor (Betz cells), interneurons (inhibitory and excitatory neurons).
Columns of the cerebral hemispheres are functional units of the cortex, divided into micromodules that have homogeneous neurons
.
Main functions
cerebral cortex:
1) integration (thinking, consciousness, speech);
2) ensuring the connection of the organism with the external environment, its adaptation to its changes;
3) clarification of the interaction between the body and systems within the body;
4) coordination of movements.
These functions are provided by corrective, triggering, and integrative mechanisms.
According to modern ideas about the localization of functions , three types of fields arise when an impulse passes through the cerebral cortex.
potential) first appeared
), disturbances in
the area of the central nuclei lead to disturbances in sensations.
2. The secondary zone lies surrounded by the nucleus, is not connected with receptors, the impulse comes from the primary projection zone along interneurons. Here, a relationship is established between phenomena and their qualities; violations lead to disturbances in perceptions (generalized reflections).
3. The tertiary (associative) zone has multisensory neurons. Information has been processed to be meaningful. System
capable of plastic restructuring and long-term storage of traces of sensory action. When violated, the form of abstract reflection of reality, speech, and purposeful behavior suffer.
Collaboration of the cerebral hemispheres and their asymmetry.
There are morphological prerequisites for the hemispheres to work together. The corpus callosum makes a horizontal connection with the subcortical formations
and the reticular formation of the brainstem.
In this way, the hemispheres work cooperatively and reciprocal innervation occurs when working together. Functional asymmetry. The left hemisphere is dominated by speech, motor, visual and auditory functions. The thinking type of the nervous
system is left-hemisphere, and the artistic type is right-hemisphere.
We will help you write any paper on a similar topic.
- Essay
Anatomy and physiology of the cerebral cortex.
From 250 rub.
- Test
Anatomy and physiology of the cerebral cortex.
From 250 rub.
- Course work
Anatomy and physiology of the cerebral cortex.
From 700 rub.
Receive completed work or specialist advice on your educational project
Find out the cost
Brain structure
The mass of the organ in an adult is approximately 1400 g. It is located in the cavity of the cranium, covered on top with membranes (soft, hard, arachnoid). We can distinguish 3 most significant parts: hemispheres, cerebellum, trunk. The hemispheres of the brain regulate higher nervous activity; they contain the departments responsible for vision, hearing, speech, and writing. The cerebellum provides balance; the brainstem contains the centers for controlling breathing and heartbeat.
Between the cerebral hemispheres there is a longitudinal fissure, in the depth of which the corpus callosum is located. The latter connects both hemispheres and allows them to coordinate each other’s work. From anatomy lessons, many remember that each hemisphere controls the opposite side of the body. It follows from this that the left hemisphere is responsible for the right half of the body.
The brain has 4 lobes (we will talk about them below). The lobes are separated by three main grooves: Sylvian, Rolandov and parieto-occipital. In addition to the grooves, the brain has many convolutions.
The brain matter itself is divided into gray (cortex) and white. The gray is made up of neurons and lines the top of the brain. The thickness of the cortex is approximately 3 mm, and the number of neurons is about 18 billion. White matter is the pathways (neurocyte fibers) that occupy the rest of the brain. It is the cortex that controls a person’s entire life from sleep to the manifestation of emotions.
Cortex
The human brain has a small top layer, about 3-4 mm thick. This is its bark - the main difference between humans and animals. It performs many functions, being used in all aspects of life. It is the action of the cortex that most affects a person’s behavior and consciousness.
Functions of the cerebral cortex include:
- Human interaction with the outside world through reflexes
- Thinking and consciousness
- Regulation of internal processes of the body, including organ function and metabolism
- Definition of human behavior
In fact, the cerebral cortex determines a person’s consciousness, controls all his thought processes, ensures interaction with the environment and the functioning of the body. It creates a relationship with the world based on reflexes, which allows a person to develop and adapt.
Each part of the cerebral cortex is determined by its functions. The limbic system is the most ancient among them. It is responsible for the regulation of behavioral reactions, the formation of sleep, emotions, memory and the control of autonomic processes.
The functions of the cortex include regulating and processing human feelings. These are sight, hearing, smell, taste and touch. Although these functions are partially divided between the cortex and midbrain.
The cerebral cortex has many functions. It is she who determines a person’s consciousness, regulates his behavior and allows him to think. It also allows you to interact with the outside world at the level of reflexes. The cortex controls organ function and metabolism. However, its functions are much broader and affect many aspects of human activity.
Functions
The functions of the temporal lobe are connected with visual, auditory, taste perception, smell, analysis and synthesis of speech. Its main functional center is located in the upper lateral part of the temporal lobe. The auditory center, the gnostic center, and the speech center are localized here.
The temporal lobes take part in complex mental processes. One of their functions is processing visual information. The temporal lobe has several visual centers, convolutions, one of which is responsible for recognizing faces. The so-called Mayer's loop passes through this temporal lobe, damage to which can result in the loss of the upper part of vision. The functions of the brain regions are used depending on the dominant hemisphere.
The temporal lobe of the dominant hemisphere of the brain is responsible for:
- word recognition;
- operates with long-term and medium-term memory;
- is responsible for assimilation of information while listening;
- analysis of auditory information and partially visual images (in this case, perception combines the visible and audible into a single whole);
- has a complex memory that combines the perception of touch, hearing and vision, while inside a person there is a synthesis of all signals and their correlation with the object;
- responsible for balancing emotional manifestations.
The temporal lobe of the non-dominant hemisphere is responsible for:
- facial expression recognition;
- analyzes speech intonation;
- regulates the perception of rhythm;
- responsible for the perception of music;
- promotes visual learning.
Brain
It is difficult to list all the functions, because this is an extremely complex organ. This includes all aspects of the human body. However, it is possible to identify the main functions performed by the brain.
The functions of the main organ include all human senses. These are vision, hearing, taste, smell and touch. All of them are performed in the cerebral cortex. It is also responsible for many other aspects of life, including motor function.
Human speech is performed in the cerebral hemispheres, namely in Broca's and Wernicke's centers. The hemispheres also perform many other functions.
The back of the brain, which includes the cerebellum, regulates balance and coordination. However, all centers important for life are located in the medulla oblongata. Here breathing, the work of the heart, blood vessels, all food and protective reflexes, as well as the regulation of muscle fibers are regulated.
Vision and hearing are not processed only in the cortex. The midbrain is also responsible for this task, regulating processes at the lower level. The same applies to motor function.
Sensitivity is regulated by the diencephalon, namely the thalamus.
The hypothalamus is the main element of the endocrine system, which regulates nerve signals and transforms them into endocrine ones. It also regulates the autonomic nervous system.
There are a lot of functions of the human brain, all of them are performed in its departments. However, most of the active activity is located in the cerebral cortex. These include hearing, smell, touch, sight and taste.
Symptoms of damage to the frontal lobe of the brain
When the nerve cells and pathways of the lobus frontalis of the brain are damaged, a motivational disorder called abulia occurs. People suffering from this disorder exhibit laziness due to a subjective loss of meaning in life. Such patients often sleep all day.
When the frontal lobe is damaged, mental activity aimed at solving problems and tasks is disrupted. The syndrome also includes a violation of the perception of reality, behavior becomes impulsive. Planning of actions occurs spontaneously, without weighing the benefits and risks, or possible adverse consequences.
Concentration of attention on a specific task is impaired. A patient suffering from frontal lobe syndrome is often distracted by external stimuli and is unable to concentrate.
At the same time, apathy occurs, loss of interest in those activities that the patient was previously interested in. When communicating with other people, a violation of the sense of personal boundaries is manifested. Possible impulsive behavior: flat jokes, aggression associated with the satisfaction of biological needs.
The emotional sphere also suffers: the person becomes unresponsive and indifferent. Euphoria is possible, which sharply gives way to aggressiveness. Injuries to the frontal lobes lead to changes in personality, and sometimes to a complete loss of its properties. Preferences in art and music may change.
With pathology of the right sections, hyperactivity, aggressive behavior, and talkativeness are observed. Left-sided lesions are characterized by general inhibition, apathy, depression, and a tendency to depression.
Symptoms of damage:
- Grasping reflexes, oral automatism.
- Speech impairment: motor aphasia, dysphonia, cortical dysarthria.
- Abulia: loss of motivation to perform.
Neurological manifestations:
- The Yanishevsky-Bekhterev grasp reflex occurs when the skin of the hand at the base of the fingers is irritated.
- Schuster reflex: grasping objects in the field of view.
- Hermann's sign: extension of the toes when the skin of the foot is irritated.
- Barre's symptom: if the arm is placed in an awkward position, the patient continues to support it.
- Razdolsky's symptom: when the hammer irritates the anterior surface of the leg or along the iliac crest, the patient involuntarily flexes and abducts the hip.
- Duff's sign: constant rubbing of the nose.
Mental symptoms
Bruns-Yastrowitz syndrome manifests itself in disinhibition and swagger. The patient lacks a critical attitude towards himself and his behavior, control over it, from the point of view of social norms.
Motivational disorders manifest themselves in ignoring obstacles to the satisfaction of biological needs. At the same time, concentration on life tasks is recorded very weakly.
Other disorders
Speech with damage to Broca's centers becomes hoarse, disinhibited, and is poorly controlled. Motor aphasia, manifested by impaired articulation, is possible.
Motor disorders manifest themselves in handwriting disorders. A sick person has impaired coordination of motor acts, which are a chain of several actions that begin and stop one after another.
Loss of intelligence and complete degradation of personality are also possible. Lost interest in professional activities. Abulistic-apathetic syndrome manifests itself in lethargy and drowsiness. This department is responsible for complex nervous functions. Its defeat leads to personality changes, impaired speech and behavior, and the appearance of pathological reflexes.
Attention!
A comment
The work of the authors under the guidance of Dr. A.A. Zueva is devoted to the surgery of intracerebral tumors of functionally significant areas of the brain (both cortical areas and pathways using the example of the pyramidal tract). The authors have accumulated sufficient clinical material (65 patients), of which 14 operations with intraoperative awakening were performed. Neurophysiology was used (a combination of bipolar stimulation and transcranial evoked potentials). All patients underwent MRI control in the early postoperative period with an assessment of the extent of tumor resection; both early and 4-month follow-up were followed in all patients.
The dependence of current strength and pulse penetration depth is analyzed in detail, and modern Russian and foreign works on this topic are presented.
A small remark that does not reduce the value of the study is a small list of references, and the second thing to mention in the work, in addition to the pyramidal tract, is the need to map the associative conductors of the white matter.
The work is of scientific and practical interest; it should, of course, be supported and the authors wish further success in their work.
S.A. Goryainov, A.A. Potapov (Moscow)
Assigned functions
The functions of the occipital lobe of the brain are associated with the analysis, perception and containment (storage) of visual information. The visual tract consists of several points:
- An eye with its retina. This paired organ is only a mechanical component of vision, performing an optical function.
- Optic nerves, through which electrical impulses directly travel at a certain frequency and carry certain information.
- The primary centers are represented by the visual thalamus and quadrigeminal.
- Subcortical and cortical centers. All of the above structures act as points of elementary perception and delivery of information. The visual cortex, in contrast, plays the role of a higher analyzer, that is, it processes the received nerve impulses into mental visual images.
It is noteworthy that the retina of the eye perceives a set of light waves, each of which has a length and consists of quanta of electromagnetic radiation. But the cortex, evolving over millions of years, “learned” to work with such signals and turn them into something more than a set of energy and impulses. Thanks to this, people have a picture of the environment and the world. Thanks to this crust, we see the elements of the universe as they appear.
The visual cortex, located on both hemispheres of the occipital lobe, provides binocular vision - the world appears three-dimensional to the human eye.
The human brain is a multifunctional structure, like each area of its cortex - therefore, the occipital lobe of the brain in a standard functional state takes little part in processing auditory and tactile signals. Under conditions of damage to neighboring areas, the degree of participation in signal analysis increases.
The visual cortex, called the association area, constantly interacts with other brain structures, forming a complete picture of the world. The occipital lobe has strong connections with the limbic system (especially the hippocampus), parietal and temporal lobes. Thus, a particular visual image may be accompanied by negative emotions, or vice versa: a long-standing visual memory evokes positive feelings.
The occipital lobe, in addition to simultaneous analysis of signals, also plays the role of an information container. However, the amount of such information is small, and most environmental data is stored in the hippocampus.
The occipital cortex is strongly associated with theories of feature integration, the essence of which is that the cortical analytical centers process individual properties of an object (color) both separately, in isolation, and in parallel.
To summarize, we can answer the question of what the occipital lobe is responsible for:
- processing visual information and integrating it into a general attitude towards the world;
- storage of visual information;
- interaction with other areas of the telencephalon and partial succession of their functions;
- binocular perception of the environment.
results
At the stage of neurophysiological mapping, the results obtained were compared with the MRI picture of the representation of functional zones, synchronized at the navigation station (Table 2).
Table 2. Results of direct electrical stimulation of the cortex in the FZZ area and white matter near the pyramidal tract
When comparing the mapping results with fMRI and tractography data, in 12 (18%) patients a wider representation of speech zones was revealed, which, in our opinion, is explained by the error in performing test tasks during fMRI and the existing preoperative neurological deficit (elements of sensory aphasia). All patients in On the 1st day after surgery, contrast-enhanced MRI control was performed (Figs. 9 and 10). Total tumor removal (100% of the tumor) was achieved in 39 (60%) patients (see Fig. 1, 9, 10), subtotal (80-95% of the tumor) - in 16 (24%), 10 (16%) patients partial removal of the tumor was performed (the tumor had invaded the internal capsule, speech centers or primary motor centers). At the time of discharge, the patients' condition on the Karnofsky scale was 80±10 points. The patient's hospital stay after surgery was 7±1 days. In 47 (72%) patients, there was no deterioration in the neurological status. In 18 (28%) patients in the early postoperative period, an increase in neurological deficit was noted in the form of an increase in paresis by 1-2 points or aggravation of speech disorders: in 11 patients the motor deficit increased by 1 point, in 7 patients the severity of aphasia increased (the group included 5 patients who did not undergo awake, and 2 patients who underwent surgery with mapping of speech zones). In 8 patients, partial regression of paresis was noted within 7 days after surgery (by an average of 1 point). When tracking the follow-up after 4 months in 18 patients in the group with increased neurological deficit, 10 of them showed regression of the neurological deficit. After 4 months, neurological deficit at the postoperative level remained in 5 patients: 3 had hemiparesis of 2-3 points, more pronounced in the arm, 3 had elements of motor aphasia, 2 had hemiparesis of 3-4 points, more pronounced in the leg. Thus, persistent neurological deficit after 4 months persisted in 8 (12%) patients, which corresponds to world literature data.
Rice. 9. Preoperative and control images: MRI of the brain, T1-weighted image with contrast, axial projection. a — preoperative image: a picture of a space-occupying formation of the left insular lobe, intensively accumulating contrast agent; b — postoperative image on the 1st day after surgery: the tumor was completely removed, there was no accumulation of contrast agent.
Rice. 10. a — preoperative images, T2-weighted image in axial projection before surgery: a volumetric formation of the left frontal lobe is determined (in the projection of Broca’s area) with pronounced perifocal edema; b — postoperative images, T-weighted image on the 1st day after radical removal of the tumor of the left frontal, insular and temporal lobes of the brain: there are no signs of residual tumor tissue.
Location
The temporal lobe is part of the telencephalon and is included in the structure of the cortex. It is located on both hemispheres of the brain on the sides below, in close contact with neighboring areas - the frontal and parietal lobes. This area of the cortex has the most pronounced boundary lines. The upper part of the temple is slightly convex, and the lower part is concave. The temporal lobe is separated from all the others by a groove called the lateral (lateral). The close location of the temporal and frontal lobes is not accidental: speech develops in parallel with thinking (frontal cortex), and these two functions are closely interconnected, since the ability to formulate and express oneself clearly (speech) is ensured by the degree of development of mental functions.
The convolutions of the temporal lobe are located parallel to the grooves that limit the area. Anatomically, there are 3 gyri: superior, middle and inferior. However, the superior cerebral fold includes 3 more small convolutions located in the sulcus itself. This group of small structures is called Heschl's convolutions. The inferior gyrus of the temple borders the transverse medullary fissure. On the lower part of the temporal lobe, in addition to the inferior gyrus, additional structures are also distinguished: the hippocampal peduncles, the lateral occipitotemporal gyrus.
B) characteristics of the sensory, motor and associative areas of the cerebral cortex
Sensory areas: the cortical ends of different analyzers have their own topography and overlap. The cutaneous receptive system is projected onto the posterior central gyrus. The visual system is in the occipital lobe (fields 17, 18, 19). The auditory system is located in the transverse temporal gyri (Heschl's gyri). The olfactory system is located in the region of the anterior end of the hippocampal gyrus (field 34). The taste system is located in the hippocampal gyrus (field 43).
Motor areas: Stimulation of the anterior central gyrus of the brain (field 4) causes a motor response. In the anterior central gyrus, the zones whose irritation causes movement are presented according to the somatotopic type, but upside down: in the upper parts of the gyrus - the lower limbs, in the lower - the upper. Anterior to the anterior central gyrus are premotor fields 6 and 8 - stereotypic movements, regulation of smooth muscle tone, plastic muscle tone through subcortical structures.
Association areas: Each association area of the cortex is connected by powerful connections to several projection areas.
In the parietal association region. The cortex forms subjective ideas about the surrounding space, about our body.
Frontal assoc. the fields have connections with the limb. department of the brain and participate in the organization of action programs during the implementation of complex motor behavioral acts. In assoc. the area receives processed information highlighting the biological significance of the signal. This allows you to formulate a program of targeted behavioral act. Assoc. region are capable of plastic rearrangements depending on the significance of incoming sensory information and store traces of sensory influences for a long time.
B) characteristics of the functional relationships of the cerebral hemispheres
Each half of the brain controls its own specific functions;
Speech and greater dexterity in the movements of the right hand are associated with the superiority of the left hemisphere in right-handed people. The left hemisphere controls “purposeful movements.”
The ability to form visual images is localized in the posterior lobes of the right brain.
The left hemisphere is responsible for verbal abilities, the right hemisphere is non-verbal.
The right hemisphere is specialized in processing information at the figurative functional level, the left - at the categorical level.
three ways of interhemispheric interactions:
1.Parallel activities. Each hemisphere processes information using its own mechanisms.
2. Electoral activities. Information is processed in the “competent” hemisphere.
3. Joint activities. Both hemispheres are involved in information processing, consistently playing a leading role at certain stages of this process.
In the right hemisphere, a more complete assessment of visual stimuli is carried out, while in the left, their most significant, significant features are assessed.
Diseases
Many researchers have found a decrease in neuronal density in the large temporal lobes of patients who have been diagnosed with schizophrenic diseases. According to research results, the right temporal lobe was larger in size compared to the left. As the disease progresses, the temporal part of the brain decreases in volume. In this case, there is increased activity in the right temporal lobe and disruption of connections between neurons of the temporal and cephalic cortex.
This activity is observed in patients with auditory hallucinations who perceive their thoughts as third-party voices. It was noted that the stronger the hallucinations, the weaker the connection between the temporal lobe and the frontal cortex. In addition to visual and auditory abnormalities, disorders of thinking and speech are added. The superior temporal gyrus in people with schizophrenia is significantly smaller than in the same region of the brain in healthy people.
According to many authors, the pathological process gradually spreads from the depths of the brain to the frontal and temporal parts, most pronouncedly manifesting itself in the superior gyrus of the right temporal lobe.
Discussion
The main goal of surgical treatment of brain gliomas is maximum resection of tumor tissue. Total or near-total removal of tumors, as well as obtaining a histological diagnosis, are key factors to improve the quality of life and increase the patient's life expectancy [5]. According to studies [6, 7], the average life expectancy of a patient after total resection of astrocytomas of I-II malignancy is on average 30 months longer than after subtotal resection (life expectancy varied from 61.1 to 90.5 months). In addition, adjuvant therapy (radiation, chemotherapy, immunotherapy) is more effective when the tumor size is small or the amount of residual tissue is small [8]. However, when the tumor is localized in the FZ of the brain, such as the motor cortex, speech areas, subcortical nuclei and internal capsule, the risk of developing neurological deficit with total removal reaches 30% [9]. Given the high risk of patient disability, it is extremely important to use all available medical technologies to perform the maximum possible tumor resection, with minimal risk of developing persistent neurological complications in the postoperative period. A detailed understanding of the relationship between the FZ and tumor tissue undoubtedly makes it possible to reduce the percentage of neurological deficits after surgery. The use of fMRI and tractography data during intraoperative navigation allows one to track the distance to the FZ in real time, but does not provide an idea of the state of functions and does not always allow one to prevent functional disorders. IONM has established itself as a method that defines the boundaries of the maximum possible functional tumor resection. Currently, neurophysiological control is actively developing and is widely used in neurosurgical practice.
The technique of intraoperative neurophysiological mapping of the cerebral cortex originates from epilepsy surgery in the first half of the twentieth century, when neurosurgeon W. Penfield and electrophysiologist H. Jasper [10] used stimulation of the cerebral cortex to localize the focus of epileptic activity. Subsequently, W. Penfield generalized the results of cortical stimulation data, obtaining an accurate representation of the motor function of different parts of the body. P. Merton and N. Morton were the first to use a non-invasive method for studying motor responses in 1980, introducing the concept of transcranial electrical stimulation. For a long time, locoregional anesthesia (pain relief based on a combination of local anesthesia along the skin incision line with the injection of a local anesthetic solution into the exit points of the sensory nerves innervating the scalp) made it possible to effectively solve the problem of pain relief for neurosurgical patients. Later, when endotracheal anesthesia was introduced into practice, this technique was forgotten and was used only in epilepsy surgery. However, in the 80s of the 20th century, thanks to the work of M. Berger and G. Ojemann [11], who introduced the concept of “cortical mapping” into surgical neuro-oncology, operations again began to include the stage of awakening the patient at the time of tumor removal. This method made it possible to prevent persistent neurological deficits in patients undergoing surgery for epilepsy. Over time, neurophysiological control techniques have improved, and different anesthesia protocols have been developed for conscious brain surgery.
According to T. Reithmeier et al. [12], the use of neurophysiological mapping of the cerebral cortex makes it possible to reduce the incidence of speech disorders after removal of intracerebral tumors by 2 times compared with the same operations without neurophysiological control - from 29 to 14%. N. Duffau et al. [13] when analyzing their material, found that the incidence of postoperative neurological disorders decreased from 17 to 6%. We managed to reduce the incidence of neurological deficits to 12%. The combination of neurophysiological monitoring with the use of the asleep-awake-asleep anesthesiological protocol makes it possible to more clearly monitor and prevent motor and speech disorders. Preoperative planning data (synchronization of fMRI with navigation MRI) does not always coincide with the data of neurophysiological mapping of the FZ. Mapping the cortex and marking functional and silent zones allows us to adjust and select the optimal area of encephalotomy with minimal risk of damage to the FZ. To directly monitor the state of the pyramidal tracts, the technique of direct subcortical stimulation is used. In this case, the strength of the stimulus is directly proportional to the depth to which it penetrates, and therefore to the distance to the motor pathways. Thus, 1 mA stimulus corresponds to approximately 1 mm [14]. Reducing the stimulus strength in the range from 10 to 3 mA makes it possible to remove the tumor as close as possible to the pathways with constant monitoring of their reactivity. According to the authors [15], this permissible distance is reduced from 8-10 to 2 mm. We used a range of 5-10 mm (5-10 mA). Subcortical stimulation was supplemented by transcranial and transcortical stimulation, which made it possible to monitor not only the reactivity of the conductors at the subcortical level, but also the continuity of the tract from the cortical level. At the same time, a decrease in the amplitude of M-responses by 50% or lower, contrary to the opinion of some authors [16], in our work did not always entail the appearance or increase of a neurological deficit. A decrease in reactivity during transcranial stimulation is explained in some cases by the effect of displacement after decompression and tumor removal, which creates an additional air gap between the cerebral cortex and the dura mater. Transcortical stimulation does not have these disadvantages. In turn, maintaining the reactivity of the pyramidal tracts at depth does not guarantee the prevention of vascular disorders near the internal capsule, which can also cause postoperative neurological deficit.
When evaluating each of the methods of preoperative planning and IONM, their inherent shortcomings are revealed, but the combination of these methods makes it possible to complement the accuracy of each of them and ultimately improve the functional outcome without sacrificing the radicality of tumor removal.
Today, IONM allows not only to prevent and detect intraoperative functional disorders, but also provides neurophysiological navigation. In combination with navigation planning in our work, this made it possible to optimize the access trajectory and perform total or subtotal removal of the FZD brain tumor with a satisfactory functional outcome in the majority of patients. Minimal or insignificant postoperative neurological deficit after subtotal tumor removal has made it possible to increase the number of patients referred for chemotherapy and radiation therapy. The main result of the work is that we were able to confirm: intraoperative mapping of the cortex and pathways with a dynamic change in stimulus strength makes it possible to obtain an idea of the location and proximity to the trajectory of the FZ intervention and stop tumor resection in time.
Assigned functions
The functionality of the temporal cortex is insignificant, however, it is highly specialized. The functions of the temporal lobe of the brain are associated with the perception, analysis and synthesis of speech, the perception of auditory information, and partly gustatory and olfactory information. Also, the location of one part of the seahorse determines another function - memory, namely its mechanical component. One area has a special purpose: Wernicke's center (sensory speech area) - located on the back of the superior temporal gyrus. This zone is responsible for the perception and comprehension of oral and written speech.
What matters is the functional asymmetry of the brain, that is, the location of the dominant areas of the cortex on the surface of the brain. This specificity of the central nervous system did not bypass the temporal lobe.
The left temporal lobe is responsible for the following functions (it should be noted that the list of tasks is based on the fact that the left hemisphere is dominant):
- Understanding audio information (music, words and speech);
- Short-term memory;
- Choice of words during a conversation;
- Synthesis of visual information with auditory information;
There is an interesting phenomenon here - synesthesia. Only 0.05% of the population has this phenomenon. The essence of the phenomenon is the ability to see the qualitative parameters of sounds in a different color spectrum. Physiologically, this is explained by the process of irradiation (spread of action potential), when the excitation of an overly irritated area of the cortex passes to the neighboring part of the brain. As a rule, famous musicians (Rimsky-Korsakov, Franz Liszt) possessed and still possess this ability. - The connection between music and emotions;
The right temporal lobe of the brain is responsible for the following functions and abilities:
- Recognition of facial expressions;
- Identification of speech intonation;
- Musical tones and rhythm;
- Memorizing and fixing visual data.
In addition to recognizing speech intonation, the non-dominant lobe also analyzes it and subsequently integrates images into the general emotional attitude towards the interlocutor. It is this part of the brain that allows a person to know whether his conversation partner is happy with him or wants to get rid of him as soon as possible.
Development of the cerebral cortex
The cortex is represented by a layer of gray matter 3-5 mm thick. There are up to 15 billion or more neurons in the cortex, and the number of gliocytes in the brain is more than 100 billion. Development. The formation of the cerebral cortex occurs through the regular migration of neuroblasts of the ependymal layer along vertically oriented radial gliocytes. The most superficial and deep layers of the cortex appear first. Then the next successive waves of migration of groups of neuroblasts arise, which differentiate into neurons of the Vth, then the IVth layer, etc. Thus, the neuroblasts of the next wave of migration overcome the layer of neurons that arose from the earlier wave of migration. This creates a layer-by-layer (screen) cytoarchitectonics of the cerebral cortex. Complex relationships are established between neurons in accordance with their place in the reflex arcs. Nuclear and screen nerve centers are formed. Close relationships during histogenesis develop between neurons and glial cells.
The EEG of infants and toddlers (i.e., up to 3 years) is characterized by the presence of θ and α rhythms with a predominance of the θ rhythm (7-8 Hz), the amplitude of the waves already reaches 80 μV. In this case, the rhythmic electrical activity of the cerebral cortex in a state of quiet wakefulness begins to be recorded from 2-3 months of postnatal life. In the intervals between series of waves with a frequency of 7-8 Hz, even higher, but rare waves with a frequency of 3-4 Hz are observed, mainly in the anterior regions of the cortex. In addition, there are always low waves with a fairly high frequency of 18-25 Hz (β rhythm).
On the EEG of preschool children (from 3 to 7 years old), two types of waves predominate: α and θ rhythm, the latter is recorded in the form of groups of high-amplitude oscillations.
The EEG of children aged 7 to 10 years is characterized by a predominance of the α-rhythm (9 Hz), however, the θ-rhythm still makes up a significant part (25\%) of the total number of oscillations.
The greater severity of the θ rhythm and paroxysmal bursts indicates a significant role of diencephalic structures in the formation of electrical activity of the brain in young children. During this age period, the activation reaction has not yet been formed [Dubrovinskaya N.V. 1985], which reflects the immaturity of the activating system of the brain. By the age of 9-10 years, paroxysmal flashes are no longer detected on the EEG of the anterior parts of the brain, the representation of the θ rhythm gradually decreases, and a mature type of activation reaction is formed.
Stabilization and acceleration of the basic EEG rhythm, a decrease in the severity of the θ rhythm, and the formation of an activation reaction in ontogenesis reflect the morphofunctional maturation of the cortex and the strengthening of its inhibitory influence on the underlying subcortical structures.
The EEG of children aged 10-12 years reveals a stable α-rhythm with the same frequency as in adults (10-12 Hz); θ-rhythm oscillations account for only about 10% of the total number of oscillations. By the age of 16-18 years, the EEG of children in all respects becomes identical to the EEG of an adult.
The entire process of EEG modification proceeds in the direction from slower low-frequency oscillations to fast high-frequency ones. In particular, a decrease in the representation of the θ rhythm with age indicates a decrease in the role of nonspecific subcortical structures in the genesis of bioelectrical activity of the brain. Increased severity during individual development of the basic rhythm of resting bioelectrical activity of the α-rhythm and the formation of its spatial organization reflect the maturation of the cerebral cortex and the functional organization of its nerve centers
Neurophysiological mechanisms of sleep and wakefulness.
According to the encephalic map, two stages of sleep are distinguished: slow or orthodox sleep (delta waves) and fast or paradoxical sleep (alpha and beta waves), which occupies 25% of the sleep duration in an adult and 58% in a newborn.
The deepest sleep is characterized by a decrease in all body functions, absence of dreams and rapid eye movements. Although this is a deep sleep, a person can quickly wake up when exposed to stimuli that are especially important to him, for example, the sound of footsteps, a child’s cry, or the creaking of doors; at the same time, he may not wake up from loud, but familiar and indifferent stimuli. I.P. Pavlov explained this phenomenon by the presence in the cerebral cortex against the background of general inhibition of “awake” centers, which he called sentry points.
When studying the electrical activity of the brain during sleep, it was noticed that periodically every 80-90 minutes, slow rhythms in the electroencephalogram are replaced by fast, high-frequency rhythms, similar to the rhythms of the waking brain. At this time, rapid eye movements are recorded, and the pulse and breathing rates increase. These are periods of so-called paradoxical sleep. Despite the fact that in paradoxical sleep the same rhythms are recorded as during active wakefulness, the perception of external signals is sharply suppressed. And waking up a person is even more difficult than during slow-wave sleep. The most important feature of paradoxical sleep is the presence of dreams. It is assumed that the “active” EEG characteristic of this phase of sleep reflects the neurodynamic processes associated with dreaming. The periodic occurrence of paradoxical sleep during night sleep is explained by the functioning of a certain neurochemical system. The destruction of the so-called blue nucleus, which contains a large amount of the neurotransmitter norepinephrine and is located in the lower part of the reticular formation of the trunk, leads to the loss of the stage of paradoxical sleep.
In general, nighttime sleep consists of cycles, and each cycle consists of five stages: one of REM sleep and four of slow-wave sleep. These periods form a biological rhythm lasting 1.5 hours. As it turned out, REM sleep, although it constitutes one part of the stages of sleep, is extremely necessary for the human body. If an adult is deprived of REM sleep for only one night, severe irritability appears. Longer absence of REM sleep can lead to mental disorders.
As a child develops, the relationship between the duration of wakefulness and sleep changes. First of all, the duration of sleep decreases. The duration of daily sleep for a newborn is 21 hours, in the second half of life the child sleeps 14 hours, at the age of 4 years - 12 hours, at 10 years -10 hours. The need for daily sleep in an adult is 7-8 hours. The formation of an electroencephalographic sleep pattern occurs in the early stages of development. All stages of sleep, including paradoxical sleep, are already expressed in infants.
Ticket number 8
Cerebral cortex, layer of gray matter 1-5 mm thick,
covering the cerebral hemispheres of mammals and humans.
This part of the brain,
which developed in the later stages of the evolution of the animal world, plays an extremely important role in the implementation of mental, or
higher nervous activity,
although this activity is the result of the work of the brain as a whole.
Thanks to bilateral connections with the underlying parts of the nervous system, the cortex can participate in the regulation and coordination of all body functions. In humans, the cortex makes up on average 44% of the volume of the entire hemisphere as a whole. Its surface reaches 1468–1670 cm2.
The structure of the cortex. A characteristic feature of the structure of the cortex is the oriented, horizontal-vertical distribution of its constituent nerve cells across layers and columns; Thus, the cortical structure is distinguished by a spatially ordered arrangement of functioning units and connections between them ( Fig. 1
)
. The space between the bodies and processes of cortical nerve cells is filled with neuroglia
and a vascular network (capillaries).
neurons
are divided into 3 main types: pyramidal (80-90% of all cortical cells), stellate and fusiform.
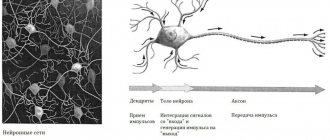
The main functional element of the cortex is the afferent-efferent (i.e., perceiving centripetal and sending centrifugal stimuli) long-axon pyramidal neuron (
Fig. 2 )
. Stellate cells are distinguished by weak development of dendrites
and powerful development
of axons,
which do not extend beyond the diameter of the cortex and cover groups of pyramidal cells with their branches.
Stellate cells play the role of perceiving and synchronizing elements capable of coordinating (simultaneously inhibiting or exciting) spatially close groups of pyramidal neurons. The cortical neuron is characterized by a complex submicroscopic structure (see Cell
)
.
Areas of the cortex that are different in topography differ in the density of cells, their size and other characteristics of the layer-by-layer and columnar structure. All these indicators determine the architecture of the cortex, or its cytoarchitectonics
The functional features of the cortex are determined by the above-mentioned distribution of nerve cells and their connections across layers and columns. Convergence (convergence) of impulses from various sensory organs is possible on cortical neurons. According to modern concepts, such a convergence of heterogeneous excitations is a neurophysiological mechanism of integrative activity of the brain, that is, analysis and synthesis of the body’s response activity. It is also significant that the neurons are combined into complexes, apparently realizing the results of the convergence of excitations on individual neurons. One of the main morpho-functional units of the cortex is a complex called a column of cells, which passes through all cortical layers and consists of cells located at the same perpendicular to the surface of the cortex. The cells in the column are closely connected to each other and receive a common afferent branch from the subcortex. Each column of cells is responsible for the perception of predominantly one type of sensitivity. For example, if at the cortical end of the skin analyzer
one of the columns reacts to touching the skin, the other to the movement of the limb in the joint.
In the visual analyzer,
the functions of perceiving visual images are also distributed across columns. For example, one of the columns perceives the movement of an object in the horizontal plane, the adjacent one in the vertical plane, etc.
The second signaling system is associated with verbal signaling, with speech. This highly sophisticated signaling system consists of the perception of words - spoken (aloud or silently), heard or seen (while reading). The development of the second signaling system has incredibly expanded and qualitatively changed the higher nervous activity of humans. The second signaling system is inextricably linked with human social life and is the result of the complex relationship in which the individual finds himself with the social environment around him. Verbal signaling, speech, language are means of communication between people; they developed among people in the process of collective work. Thus, the second signaling system is socially determined.
Outside society - without communication with other people - the second signaling system does not develop. Cases have been described in which children carried away by wild animals remained alive and grew up in an animal den. They did not understand speech and could not speak. It is also known that people who, at a young age, were isolated for decades from the society of other people, forgot their speech; their second alarm system stopped functioning.
The second signaling system, according to Pavlov, “the highest regulator of human behavior”, prevails over the first and to some extent suppresses it. At the same time.
Ticket number 9
Symptoms of the lesion
When the area responsible for vision is affected, the following symptoms are observed in the clinical picture:
Dyslexia is the inability to read written words. Although the patient sees the letters, he cannot analyze and understand them.
Visual agnosia: loss of the ability to distinguish objects in the environment by their external parameters, but patients manage to do this by touch.
Impaired visuospatial orientation.
Impaired color perception.
Hallucinations are the visual perception of something that does not exist in the real objective world. In this case, the characteristics of photopsia are lightning-fast color perception and various types of flashes.
Visual illusions are a distorted perception of real-life objects. For example, the patient may perceive the world in red colors, or all surrounding objects may seem extremely small or large to him.
When the inner surface of the occipital cortex is damaged, loss of the opposite visual fields is observed.
With large-scale tissue damage in this area, complete blindness may occur.
Didn't find a suitable answer? Find a doctor and ask him a question!
Consequences of damage
The occipital lobes are connected to the parietal lobes and help them through the work of the visual centers. Interaction with frontal neurons contributes to logical thinking, learning languages, mathematics, perception of topographic objects and navigation among them. Damage to one area can affect the course of the entire process.
The parietal lobes of the brain may lose their functions due to injury, ischemic or hemorrhagic stroke, tumor growth, or metastases from other organs (breast).
Since this most important and extensive part of the central nervous system is responsible for a large number of functions (sensitivity, skills, coordination of movements), and also actively interacts with other areas, when it is damaged, serious, often irreversible disorders develop.
The consequences of the lesion depend on its area and location. There are three main clinical syndromes:
- Gerstmann's syndrome. Occurs with injuries, tumor development, hemorrhage in the left parietal lobe. As a result, the patient loses the ability to perform mathematical calculations, perceive oral and written speech, and logical thinking. The following symptoms appear: acalculia, alexia, agraphia, agnosia (impaired recognition) of fingers.
- Balint's syndrome. Occurs when both parietal lobes are damaged - left and right. This leads to loss of motor skills and visual attention. A person becomes incapable of holistic visual perception, and voluntary eye movements are weakened. The ability to evaluate the parameters of an object by touch or perform any actions with it is lost.
- Right-sided lesion. The patient becomes unable to take full care of himself, as he does not notice half of his body (anosognosia). Drawing skills deteriorate significantly, and constructive apraxia develops.
Kinesthetic apraxia is a violation of practical skills associated with an incorrect assessment of the efforts required to move objects and other manipulations with them. Man is unable to calculate force. Movements become rough and clumsy.
Damage to the lower parts leads to ideomotor and ideator apraxia - loss of the ability to perform actions on command. When the non-dominant hemisphere is damaged, anosognosia develops - ignoring the half of the body that has undergone paralysis (hemiplegia) and loss of sensitivity (hemianesthesia).
The angular gyrus is responsible for reading, writing, arithmetic skills, and distinguishing between the left and right halves of the body. When it is damaged, these functions suffer.
Symptoms of the lesion include homonymous and inferior quadrant hemianopsia. This is loss of the visual field, disappearance of natural nystagmus, ataxia, loss of topographic memory, spontaneous pain, hallucinations, apraktoagnosia (ignoring the loss of skills on one side of the body), tactile agnosia.
Conclusion
If a person experiences the symptoms described above, it is necessary to seek medical help and undergo diagnostics: MRI of the brain, echoEG, electroencephalogram. Disturbances can be caused by hemorrhage, head injury, and diseases of the central nervous system.
Attention!
Material and methods
In the period from 2014 to 2015, in the Department of Neurosurgery No. 2 of the National Medical Center named after.
N.I. Pirogov treated 65 patients (43 (66%) men and 22 (34%) women aged 32 to 68 years) with glial tumors of the brain. During the initial neurological examination, motor deficits of varying severity were detected in 46 (71%) patients (6 patients were diagnosed with hemiparesis with a decrease in strength to 1 point, in 15 - to 2-3 points, in 25 - to 4 points). 17 (26%) patients were diagnosed with aphasia (12 of them had a combination of speech and motor disorders, 5 had isolated speech disorders). In 40 (62%) patients, tumors were localized in the frontal and temporal lobes. Isolated damage to one lobe was present in only 9 patients: insular in 4, frontal in 2, and temporal in 3. In 37 (58%) patients, the tumor affected the left hemisphere, and in 24 (36%) - the right. In 4 (6%) patients, the tumor spread to both hemispheres of the brain (Table 1).
Table 1. Localization of glial tumors in operated patients
64 patients underwent primary surgery. One patient was operated on 2 times during the observation period: initially for a tumor of the frontal, temporal and insular lobes on the left (involving Broca's area and Wernicke's area) and again 16 months later due to continued growth of the tumor. Both operations were carried out using the asleep-wake-asleep protocol. Control of the radicality of tumor removal (MRI with contrast) was performed in all patients on the 1st day after surgery (Fig. 1).
Rice. 1. Images of preoperative planning at the navigation station. MRI brain, T1-weighted image with contrast. a - frontal; b - sagittal; c — axial projection. A space-occupying formation (1) of the left temporal and parietal lobes of the brain (in the projection of the superior temporal, angular and supramarginal gyri) with fuzzy, uneven contours, with pronounced perifocal edema, intensively accumulating contrast agent is determined. Arrows indicate the motor cortex (2), pyramidal tracts (3) and speech areas (4); d — 3D model of the brain with projection of the FZ and tumor.
Along with MRI in standard modes, 50 (77%) patients underwent fMRI at the stage of preoperative diagnosis due to the presence of speech disorders in 17 patients and involvement of the internal capsule in 4 patients (in addition, the group included 9 patients who had no manifestations of aphasia , but the risk of its development after surgery was high). The fMRI technique is based on recording regional hemodynamic changes that occur when the cerebral cortex is activated in response to specific stimulation (alternating phases of rest and motor, mental or other activity). Based on the results of the examination, the relationship of the tumor with the motor pathways, Wernicke’s and Broca’s areas was established in these patients (Fig. 2 and 3).
Rice. 2. Images from the navigation station MRI of the brain, T1-weighted image with contrast, sagittal (a) and axial (b) projections: a volumetric formation is determined (1) in the right temporal and parietal lobes of the brain, with fuzzy uneven contours, with pronounced perifocal swelling, intensively accumulating contrast agent. The pyramidal tracts (2) passing anterior to the tumor are indicated; c — 3D model of the spatial relationship of the tumor (1) and pyramidal tracts.
Rice. 3. Preoperative and control images MRI of the brain, T2-weighted image, sagittal and frontal projections. Preoperative T2 (a) and Flair (b) images: a picture of a space-occupying lesion in the left frontal lobe involving the premotor area and the anterior parts of the precentral gyrus; postoperative T1 (c) and Flair (d) images on the 1st day after surgery. The tumor was completely removed.
In patients with frontotemporal tumor localization in the dominant hemisphere and proximity to speech centers, in order to reduce the risk of the appearance or increase of postoperative motor, sensory and amnestic aphasia, tumor removal was carried out with intraoperative awakening (according to the asleep-awake-asleep protocol) (16 patients). For this purpose, a team of anesthesiologists and neurosurgeons had a conversation with the patient on the eve of the operation, during which all stages of the future surgical intervention were considered. Particular attention was paid to the moment of awakening in the operating room. The anesthesiologist sought to ensure that the patient had a conscious understanding of what he would see in the operating room. It was discussed what sensations he would experience when he woke up, what the peculiarities might be when waking up. In addition, testing with pictures was carried out, during which the patient named and described the objects depicted, and also practiced mental counting, memorizing a sequence of words, and reading. The criteria for selecting patients for the asleep-awake-asleep protocol were the absence of pronounced mnestic disorders, i.e., the ability to enter into full verbal contact, the absence of pronounced mental lability, and the absence of gross motor and sensory speech deficits. During testing, obvious mnestic disturbances or pronounced sensorimotor aphasia were revealed in 5 patients, as a result of which they decided to refrain from performing a conscious craniotomy.
During the operations, IONM was performed using the Natus Xltek protektor apparatus. The purpose of IONM is to dynamically monitor spontaneous and evoked bio-electrical activity of the brain (motor evoked potentials). During neurophysiological monitoring, motor evoked potentials were assessed using transcranial electrical stimulation based on the activation of pyramidal cells of the corticospinal tract (Brodmann area 4 of the precentral gyrus). Stimulating electrodes were located in the projection of points C3, C4, according to the international scheme 10-20 [3]. Depending on the surgical approach, different electrode placement options were used. To assess the conduction of electrical impulses along the pyramidal tracts, all patients underwent transcranial electrical stimulation, regardless of the severity of the neurological deficit. Motor responses were recorded using needle electrodes installed in muscles ( m .
Orbicularis Oculis , m . Orbicularis Oris , m . Deltoideus , m . Thenari / Hypothenari , m . Rectus Femori , m . Tibialis Anterior
). Transcranial stimulation (Fig. 4) was performed in single trains of 4 short high-frequency stimuli (500 Hz). Tension parameters were selected individually until representative M-responses were obtained from all tested muscles. Registration of M-responses was carried out under conditions of amplifier sensitivity of 50 μV/div with a notch filter of 50 Hz. During the operation, motor responses were recorded on both sides. The difference in amplitude and latency varied depending on the initial neurological deficit and options for installing stimulating electrodes.
Rice.
4. Monitoring of the pyramidal tracts (transcranial stimulation) during removal of glioma of the lower parts of the precentral gyrus of the frontal and lower parts of the postcentral gyrus of the parietal lobe of the left hemisphere. The test muscles were chosen. Deltoideus (a), m. Thenari (b, c), m. Tibialisanterior(d, d). The orange arrow indicates the M-response obtained from the muscle being tested. The red arrow indicates a series of stimuli. Motor cortical mapping (Fig. 5) was used in 50 patients with involvement of the precentral gyrus or premotor cortex. For this purpose, the technique of direct stimulation of the cortex with a bipolar electrode was used in packs of 4 stimuli with an internal frequency of 500 Hz and a stimulus strength of up to 25 mA with registration of motor responses from the tested muscles of the contralateral side.
Rice. 5. Motor mapping of the middle and lower parts of the precentral gyrus before encephalotomy in a patient undergoing removal of a glioma of the frontotemporal localization. The test muscles chosen were m. Longinalis superior (a), m. Orbicularis oris (b), m. Deltoideus (c), m. Thenari (g), m. Tibialis Anterior (e), m. Rectus.
Patients ( n
=16) with the tumor localized in the projection of the speech zones, tumor removal was carried out according to the asleep-awake-asleep protocol [4]. After depression of consciousness by intravenous administration of a propofol solution at a dose of 1.0-1.5 mg/kg, analgesia with a fentanyl solution at a dose of 2.5-3.0 mcg/kg and muscle relaxation with rocuronium at a dose of 0.7 mg/kg, tracheal intubation was performed and mechanical ventilation began in normal ventilation modes. Control of the patient's level of consciousness was ensured by inhalation of desflurane in doses of 0.3-0.6 MAC under conditions of monitoring the depth of depression of consciousness (target BIS values were 50-60). To assess the level of muscle relaxation, a neuromuscular conduction monitor using the TOF technique was used. The skin incision line was infiltrated with a solution of 0.2% ropivocaine in total doses not exceeding 300 mg, taking into account regional anesthesia. Anesthesia of the dura mater (DRM) was carried out by applying pads with lidocaine. After craniotomy was performed and the level of restoration of neuromuscular conduction, TOF 0.9 or more, was achieved, the supply of desflurane was stopped, the patient was awakened and extubated. Mapping of the FZZ of the brain was performed in 2 stages. Before awakening the patient, the motor areas bordering the formation were verified using direct electrical stimulation of the cortex. After awakening and extubation, verbal contact was established, and then speech zones were mapped (Fig. 6). For intraoperative verification of Wernicke's area, tasks were selected to repeat a series of frequency words in threes, which allows diagnosing disorders of phonemic hearing and the volume of auditory-verbal perception (as well as the pronunciation side of speech), testing with naming pictures, reading and counting. The intraoperative speech testing procedure was practiced with patients on the eve of surgery; only tasks that were available for stable, error-free execution were included in the test set. During stimulation of the cortex with a bipolar stimulator in Broca's and Wernicke's areas with rhythmic bursts of 4 stimuli with a strength of 15-20 mA, various types of speech impairment were recorded in some patients: speech-arest (5 patients), elements of motor aphasia, literal paraphasia with replacement of sounds by acoustic proximity and verbal paraphasia with substitution of words based on acoustic proximity, characteristic of phonemic hearing impairment (7).
Rice.
6. Intraoperative mapping of speech zones. Intraoperative photo (a). The trepanation window is formed in the left frontal-temporo-parietal region. The dura mater has been opened. After the patient woke up, mapping of speech zones was performed. Broca's area (22, 21, 25 - yellow outline), Wernicke's area (16-18, 20 - green outline) and the lower parts of the precentral gyrus (22, 26 - blue outline) were identified. On fMRI (b), the speech centers are indicated in green; the tumor is localized in the left insula. After verification of Broca's and Wernicke's areas, the tumor was removed with neurological and neurophysiological control of the preservation of speech functions and motor tracts (Fig. 7). In 2 patients, after mapping of speech zones, motor restlessness and emotional lability developed, which required resumption of endotracheal anesthesia (average time awake was 30±12 minutes).
Rice. 7. Intraoperative photo. Stage of tumor removal with intraoperative mapping of speech zones. At the awake stage, mapping of speech zones was carried out. The marks indicate Wernicke's area, discovered during direct stimulation of the cortex during the awakening stage. The green outline indicates the projection of the tumor.
In the remaining 14 patients, testing continued throughout the entire tumor removal (awake time was 120±20 minutes). After tumor removal, patients were again anesthetized, intubated with brief muscle relaxants, and surgery was completed under general anesthesia with continued monitoring via transcranial stimulation.
In 11 (17%) patients with tumor spread into the internal capsule, stimulation of the motor pathways was performed (Fig. 8). The stimulation threshold was decreased stepwise from 10 to 5 mA (according to the literature, a change of 1 mA corresponds to a change of distance of 1 mm). Changing the stimulus strength to a minimally representative one made it possible to remove the tumor in close proximity to the internal capsule. In 5 (8%) patients during tumor removal due to the appearance of a motor response to a stimulus strength of 5 mA, removal was stopped due to the extremely high risk of neurological deficit.
Rice. 8. Removal of a frontal lobe tumor with intraoperative mapping of motor areas. a — intraoperative photo: the stage of tumor removal of the left frontal lobe, the arrow indicates a bipolar stimulator used during mapping of motor pathways in the white matter. On fMRI, arrows indicate the motor representation of the arm (b) and leg (c), the tumor is located in close proximity to these zones and is in contact with the pyramidal tracts.
Regardless of the tumor location and the chosen anesthesia protocol (including awake craniotomy), all patients underwent background monitoring of transcranial motor evoked potentials. In 8 patients, the amplitude of the M response decreased by more than 50% during tumor removal. When assessing the postoperative neurological status, all of them were included in a group of 11 patients whose motor deficit increased. In 21 patients, a temporary decrease in amplitude was noted (by no more than 40%), which is apparently explained by the presence of a brain displacement effect after tumor removal or the effect of short muscle relaxants at the stage of re-intubation according to the asleep-awake-asleep protocol.
In 43 (66%) patients, the histological diagnosis corresponded to glioblastoma (WHO Grade IV), in 7 (11%) - fibrillary astrocytoma (WHO Grade II), in 6 (9%) - oligodendroglioma (WHO Grade II). Anaplastic astrocytoma (WHO Grade III) was verified in 9 (14%) patients, of which 2 patients were re-operated using mapping due to continued tumor growth.
Motor zone
Let's talk about the motor zone separately. It should be noted that this zone of the cortex does not correlate in any way with the lobes discussed above. It is part of the cortex containing direct connections to motor neurons in the spinal cord. This name is given to neurons that directly control the activity of the muscles of the body.
The main motor area of the cerebral cortex is located in a gyrus called the precentral gyrus. This gyrus is a mirror image of the sensory area in many aspects. Between them there is contralateral innervation. To put it another way, the innervation is directed to the muscles that are located on the other side of the body. The exception is the facial area, which is characterized by bilateral control of the muscles located on the jaw and lower part of the face.
Slightly below the main motor zone is an additional zone. Scientists believe that it has independent functions that are associated with the process of outputting motor impulses. The supplementary motor area has also been studied by specialists. Experiments carried out on animals show that stimulation of this zone provokes the occurrence of motor reactions. The peculiarity is that such reactions occur even if the main motor area has been isolated or completely destroyed. It is also involved in motor planning and speech motivation in the dominant hemisphere. Scientists believe that if the accessory motor is damaged, dynamic aphasia can occur. Brain reflexes suffer.
Sensory, motor and associative areas of the cortex.
| Random page | VOLUME-1 | VOLUME-2 | VOLUME-3 Architecture | Biology | Geography | Other | Foreign languages |
| Computer science | Story | Culture | Literature | Mathematics |
| Medicine | Mechanics | Education | Occupational Safety and Health | Pedagogy |
| Policy | Right | Programming | Psychology | Religion |
| Sociology | Sport | Construction | Physics | Philosophy |
| Finance | Chemistry | Ecology | Economy | Electronics |
Question No. 12. Structural overview of the spinal cord. | The structure of the reflex arc. | Question No. 14. Ascending and descending projection paths. | Structural overview of the medulla oblongata | Structural overview of the hindbrain | Cerebellum, structure and functions | Question No. 18. Structural overview of the midbrain. | Question No. 19. Structural overview of the diencephalon. | Question No. 20. Structural overview of the forebrain. | Hippocampus Structure and functions. |
Characteristics of functional specialization.
Between the hemispheres there is a division of responsibility for speech, memory, emotional tone and emotional coloring of tasks and behavior, elements and types of thinking.
| Left hemisphere | Function | Right hemisphere |
| Perception and reproduction semantic signals: 1) Speech perception center at VVI (Wernicke center). If the patient hears but does not understand, control over the content of speech is also impaired. 2) Reading center - meaning analyzer (angular gyrus). 3) The center of pronunciation is Broca’s center (II and III frontal gyri). If it is violated, he understands, but cannot speak. 4) The writing center is the middle frontal gyrus, its posterior section. | Speech | Perception of semantic signals, playback control: 1) Perception of the semantic load of speech, creation of melodies. 2) Perception of intonation characteristics (the sound of rain). 3) Intonation coloring of speech. 4) Moderates excessive speech activity. |
| To abstract phenomena. Verbal and computer archive. If there is a violation, the patient does not remember the year, date, month. | Memory | On figurative phenomena . If impaired, does not recognize specific images (test - cannot add the missing part to the picture), does not orientate in a visual situation. |
| Positive emotional tone: 1) good health; 2) friendliness with people, sociable, optimistic; 3) feelings are distinguished by restraint and moderation. | Emotions | Negative emotional tone. 1) acute perception of the world and phenomena - they feel sensitively, prone to emotionally charged experiences; 2) with increased activity, complaints about well-being, gloomy mood, pessimism. |
| Abstract-logical. 1) penchant for analysis: a) organize and systematize chaos and confusion; b) operating principle – from general to specific; c) gravitate towards theoretical activity, high sense of purpose, ability to predict events (“creators” and “destroyers” (Ehrenfest). | Elements of thinking | Figurative. 1) Tend to be contemplative in life. 2) They gravitate towards specific types of activities. |
| The type of “thinker”, since abstract-logical thinking predominates. | Thinking type | The type is “artistic”, since concrete sensory thinking predominates. |
Up to 80% of people are of the average type. Why? The answer to this question is given by analysis of the material on asymmetry in the activity of the hemispheres.
Asymmetry in the activity of the hemispheres.
It is known that the hemispheres are connected to each other through the corpus callosum. These are bundles of white matter that connect the hemispheres, as a result of which coordination of their activities becomes possible.
Functions of the cerebral cortex
Previously, it was believed that the higher functions of the human brain are carried out by the cerebral cortex. Even in the last century, it was found that when the cortex is removed from animals, they lose the ability to perform complex acts of behavior determined by acquired life experience. It has now been established that the cortex is not the highest distributor of all functions. Many of its neurons are part of the middle-level sensory and motor systems. The substrate of higher mental functions is the distribution systems of the central nervous system, which include both subcortical structures and cortical neurons. The role of any area of the cortex depends on the internal organization of its spinal connections, as well as its connections with other formations of the central nervous system. At the same time. In humans, in the process of evolution, corticolization occurred of all, including vital visceral functions. Those. their subordination to the cortex. It has become the main integrating system of the entire central nervous system. Therefore, in the event of the death of a significant part of the cortical neurons in a person, his body becomes non-viable and dies as a result of a violation of homeostasis (brain hypothermia). The cerebral measles consists of six layers:
I. Molecular layer, uppermost. Formed by many ascending dendrites of pyramidal neurons. There are few neuron bodies in it. This layer is pierced by axons of nonspecific nuclei of the thalamus belonging to the reticular formation. Due to this structure, the layer ensures activation of the entire cortex.
2-Outer granular layer. It is formed by densely located small neurons that have numerous synaptic contacts with each other. Due to this, a long-term circulation of nerve impulses is observed. This is one of the memory mechanisms.
3. Outer pyramidal layer. Consists of small pyramidal cells. With the help of them and the cells of the second layer, intercortical connections are formed, i.e. connections between different areas of the cortex.
4. Inner granular layer. Contains stellate cells on which the axons of switching and associative neurons of the thalamus form synapses. All information from peripheral receptors comes here.
5. Inner pyramidal layer. Formed by large pyramidal neurons, the axons of which form descending pyramidal tracts leading to the medulla oblongata and spinal cord.
6. Layer of polymorphic cells. The axons of its neurons go to the thalamus.
Cortical neurons form neural networks that include three main components:
1. afferent or input fibers.
2. interneurons
3. efferent - output neurons. These components form several layers of neural networks.
1. microgrids. The lowest level. These are individual interneuron synapses with their pre- and postsynaptic structures. A synapse is a complex functional element that has internal self-regulatory mechanisms. Cortical neurons have highly branched dendrites. They contain a huge number of spines in the form of drumsticks. These spines serve to form input synapses. Cortical synapses are extremely sensitive to external influences. For example, deprivation of visual stimulation by keeping growing animals in the dark leads to a significant reduction in synapses in the visual cortex. In Down's disease, there are also fewer synapses in the cortex than normal. Each spine, forming a synapse, acts as a transducer of signals going to the neuron.
2. Local networks. The neocortex is a layered structure, the layers of which are formed by local neural networks. Impulses from all peripheral receptors can come to it through the thalamus and olfactory brain. Input fibers pass through all layers, forming synapses with their neurons. In turn, collaterals of input fibers and interneurons of these layers form local networks at each level of the cortex. This structure of the cortex provides the ability to process, store and interact with various information. In addition, there are several types of output neurons in the cortex. Almost every layer of it produces output fibers that go to other layers or distant areas of the cortex.
3. Cortical columns. Input and output elements with interneurons form vertical cortical columns or local modules. They pass through all layers of the cortex. Their diameter is 300-500 microns. The neurons that form these columns are concentrated around the thalamo-cortical fiber, which carries a certain type of signal. The columns contain numerous interneuron connections. Neurons of layers 1-5 of the columns provide perception and processing of incoming information. Neurons of layers 5-6 form the efferent pathways of the cortex. Adjacent columns are also interconnected. In this case, the excitation of one is accompanied by inhibition of the neighboring ones. Columns performing the same type of function are concentrated in certain areas of the cortex. These areas are called cytoarchitectonic fields. There are 53 of them in the human cortex. The fields are divided into primary, secondary, and tertiary.
Primary ones provide processing of certain sensory information.
Secondary and tertiary interaction of signals from different sensory systems. In particular, the primary somatosensory field, to which impulses from all skin receptors (tactile, temperature, pain) go, is located in the region of the central posterior gyrus. The most space in the cortex is occupied by the lips, face, and hands. Therefore, when this area is damaged, the sensitivity of the corresponding areas of the skin changes. Representation of proprioceptors of muscles and tendons, i.e. The motor cortex occupies the anterior central gyrus. Impulses from the proprioceptors of the lower extremities go to the upper part of the gyrus. From the muscles of the torso to the middle part. From the muscles of the head and neck to its lower part. The largest area of this field is also occupied by the muscles of the lips, tongue, hands and face.
Impulses from the receptors of the eye enter the occipital regions of the cortex near the calcarine sulcus. Damage to the primary fields leads to cortical blindness, and damage to the secondary and tertiary fields leads to loss of visual memory. The auditory cortex is located in the superior temporal gyrus and the transverse gyrus of Heschl. When the primary fields of the zone are damaged, cortical deafness develops. Peripheral - difficulties in distinguishing sounds. In the posterior third of the superior temporal gyrus of the left hemisphere there is a sensory center for speech - Wernicke's center. With its pathological changes, the ability to understand speech is lost. The motor center of speech, Broca's center, is located in the inferior frontal gyrus of the left hemisphere. Abnormalities in this part of the cortex lead to loss of the ability to pronounce words.
Functional asymmetry of the hemispheres.
The forebrain is formed by two hemispheres, which consist of identical lobes. However, they play different functional roles. The differences between the hemispheres were first described in 1863 by the neurologist Paul Braka. who discovered that with tumors of the left frontal lobe the ability to pronounce speech is lost. In the 50s of the 20th century, R. Sperry and M. Gazzaniga studied patients in whom the corpus callosum was transected in order to stop epileptic seizures. It contains commissural fibers connecting the hemispheres. The mental abilities of people with split brains do not change. But with the help of special tests it was discovered that the functions of the hemispheres are different. For example, if an object is in the field of vision of the right eye, then visual information enters the left hemisphere, then such a patient can name it and describe its properties. read or write the text.
If an object falls into the field of vision of the left eye, then the patient cannot even name it and talk about it. He can't read with this eye. Thus, the left hemisphere is dominant in relation to consciousness, speech, counting, writing, abstract thinking, and complex voluntary movements. On the other hand, although the right hemisphere does not have pronounced speech functions, it is to a certain extent capable of understanding speech and thinking abstractly. But to a much greater extent than the left, it has mechanisms for sensory recognition of objects of figurative memory. The perception of music is entirely a function of the right hemisphere. Those. the right hemisphere is responsible for non-speech functions, i.e. analysis of complex visual and auditory images, perception of space and shape. Each hemisphere separately receives, processes and stores information. They have their own feelings, thoughts, and emotional assessments of events. The left hemisphere processes information analytically, i.e. sequentially, and the right one simultaneously, intuitively. those. hemispheres use different ways of knowing. The entire education system in the world is aimed at developing the left hemisphere, i.e. abstract thinking rather than intuitive. Despite the functional asymmetry, normally the hemispheres work together, providing all processes of the human psyche.
Plasticity of the cortex.
Some tissues retain the ability to form new cells from progenitor cells throughout life. These are liver cells, skin enterocytes. Nerve cells do not have this ability. However, they retain the ability to form new processes and synapses, i.e., each neuron is capable of forming new ones when a process is damaged. Restoration of processes can occur in two ways: through the formation of a new growth cone and the formation of collaterals. Typically, the growth of a new axon is prevented by the appearance of a glial scar. But despite this, new synaptic contacts are formed along the collaterals of the damaged axon. The plasticity of cortical neurons is highest. Any of its neurons is programmed to actively try to restore lost connections when damaged. Each neuron is involved, and competes with others to form synaptic contacts. This serves as the basis for the plasticity of neural cortical networks. It has been established that when the cerebellum is removed, the nerve pathways leading to it begin to grow into the cortex. If a section of the brain of another animal is transplanted into an intact brain, the neurons of this piece of tissue form numerous contacts with the neurons of the recipient’s brain.
The plasticity of the cortex manifests itself as under normal conditions. For example, during the formation of new intercortical connections during the learning process, and during pathology. In particular, the functions lost due to damage to a part of the cortex are taken over by its neighboring fields or another hemisphere. Even when large areas of the cortex are damaged due to hemorrhage, their functions begin to be performed by the corresponding areas of the opposite hemisphere.
Electroencephalography. Its significance for experimental research and clinical practice.
electroencephalography (EEG is a recording of the electrical activity of the brain from the surface of the scalp. For the first time, a human EEG was recorded in 1929 by the German psychiatrist G. Berger. When taking an EEG, electrodes are applied to the skin, the signals from which are amplified and sent to an oscilloscope and writing device. Normal The following types of spontaneous oscillations are recorded:
1. a-rhythm. These are waves with a frequency of 8-13 Hz. Observed in a state of wakefulness, complete rest and with eyes closed. If a person opens his eyes, the a-rhythm is replaced by the p-rhythm. This phenomenon is called a-rhythm blockade.
2. B-rhythm, Its frequency is from 14 to 30 Hz. It is observed during an active state of the brain and is read as the intensity of mental work increases.
3. (gama) - rhythm. Oscillations with a frequency of 4-8 Hz. Registered while falling asleep.
superficial sleep and shallow anesthesia.
4. (sigma) - rhythm. Frequency 0.5-3.5 Hz. Observed during deep sleep and anesthesia.
The lower the frequency of EEG rhythms, the greater their amplitude. In addition to these basic rhythms, other EEG phenomena are recorded. For example, as sleep deepens, sleep spindles appear. This is a periodic increase in the frequency and amplitude of the theta rhythm. When waiting for a command to action, a negative E-wave of anticipation arises, etc.
In experiments, EEG is used to determine the level of brain activity, and in the clinic to diagnose epilepsy (especially latent forms), as well as to detect brain death (cortex lives 3-5 minutes, stem neurons 7-10, heart 90, kidneys 150).
Functions
In addition to the fact that the cortex has motor, sensory and associative zones, it is all responsible for the functioning of parts of the brain. Each zone consists of its own special neurons (pyramidal, basket-shaped, stellate, fusiform, etc.).
Based on their functions, neurons are divided into the following types:
- Insert. Participate in the processes of excitation and inhibition.
- Afferent. These are the famous stellate neurons. They receive impulses that come from the periphery (visual, auditory, tactile, etc.). They also participate in the formation of sensations. These cells transmit incoming impulses to efferent and intercalary neurons. It is curious that there are polysensory neurons that are capable of picking up different impulses from the visual thalamus.
- Efferent. These are large pyramidal cells that are responsible for transmitting impulses to the periphery, where they provide certain activities. Damage to this zone cuts off communication with certain sensory organs.
Biology lesson “Structure of the cerebral cortex”
Development of an open biology lesson for 8th grade students on the topic
"Structure of the cerebral cortex."
Raevskaya Evgenia Yurievna, biology teacher
The purpose of the lesson:
Show the structure and significance of the cerebral cortex.
Lesson objectives:
- Give biological concepts on the structure and significance of the cerebral cortex;
- Ensure the acquisition of knowledge about the structural features of the brain;
- Show that the cerebral cortex is the basis of human mental activity;
- Show hereditary disorders of the nervous system and brain.
Literature:
- Balabanova V.V. and others. Open lessons in biology. 7-9 grades. – Volgograd: Teacher, 2003.
- Kuzmina I.D. Biology. Man.9th grade: Methodological manual for the textbook, ed. A.S. Batueva “Biology. Human. 9th grade” - M.: Bustard, 2000.
- Rokhlov V.S. School workshop. Biology. Man. 9th grade. -2nd ed., stereotype. – M.: Bustard, 2000.
- Zverev I.D. Reading book on human anatomy, physiology and hygiene: A manual for students of grade 9. avg. school – 4th ed., revised. – M.: Education, 1989.
Equipment and materials:
- Printed manuals (tables on the nervous system).
- Demountable models of the brain.
- Cards for monitoring students' knowledge.
During the classes
I. Organizational moment
(Preparation of students for the lesson, topic and course of the lesson.)
II. Repetition of what has been covered (homework)
Frontal survey of students on the topic: “The brain and its parts.”
Questions
:
- Where is the human brain located7
- What parts does the brain consist of?
- What does the hindbrain include?
- What function does the midbrain perform?
- What are the functions of the medulla oblongata?
– Continue the sentence (on cards 1) – students read aloud.
- Nervous regulation of physiological processes consists in the interaction of body organs with the help of ___________
- The nervous system is divided into two parts: ______________________________
- Clusters of neuron cell bodies form the _______________ of the brain and spinal cord.
- The bodies of nerve cells can also lie outside the central nervous system, near internal organs or in their walls, forming here ______________________________
- An electrical wave traveling along a nerve fiber is called ______________________
- The body's response to irritation of sensitive formations - receptors, carried out with the participation of the nervous system is _________________..
- The forebrain consists of the diencephalon and_____________________
Game moment - laboratory experiment No. 1 - The work of the diencephalon of students.
All the guys do exercises, and then the teacher suddenly loudly gives the command “FREEZE.” Students freeze in different positions (postural reflex of the diencephalon).
Teacher:
Who will show the parts of the brain on the poster?
(A student comes to the board.)
We conclude that the brain consists of ________ sections and the cerebral cortex - the topic of our lesson!
III. Learning new material
Writing in a notebook is the topic of the lesson. Write a lesson plan on the board.
Plan:
- The structure of the cerebral cortex.
- The main lobes of the cerebral cortex and their functions. (page 31-32).
- Damage to the cerebral cortex, hereditary disorders.
Teacher:
The cerebral hemispheres of the forebrain are the largest formation of the brain. They are covered on top with gray matter - bark, which forms many folds, grooves and convolutions. The folded structure increases the surface of the cortex and its volume, and therefore the number of its neurons. In humans, it contains approximately 14 billion nerve cells. Accumulations of gray matter are also located under the cortex in the depths of the hemispheres. Various subcortical nuclei are located here.
The cerebral cortex is the highest division of the central nervous system. It is responsible for the perception of all information received by the brain and for the control of all complex muscle movements. It is with the functions of the cortex that mental and speech activity and memory are associated. (show this department on the poster)
Scheme on the board:
CNS—— 2. brain ——— 3. cerebral cortex — 4. gray matter
The cerebral cortex consists of four lobes:
1. FRONTAL. 2. PARIETAL. 3. TEMPORAL. 4. OCCIPITAL.
(Shows on the board - on the poster.)
The main lobes of the cerebral cortex and their functions.
Independent work in pairs. (time – 5 minutes to select objects).
Completing the table in the workbooks (pp. 31–32). Self-control.
See page 33.
Teacher:
Damage to the cerebral cortex - hereditary disorders occur when:
- traumatic situations (skull fracture)
- impaired blood supply to the gray matter (hematomas - strokes)
- hereditary disorders - can be caused by environmental factors, the combination of chromosomes of the parents, diseases suffered by the mother during pregnancy.
– DOWN'S disease
– the presence of 3 chromosomes instead of 2 in the 21 pairs of human chromosomes = dementia, reduced learning ability.
– Mental retardation
– dementia, occurs when an increase or loss of the X chromosome in women, a gene mutation.
– Meningitis
- caused by bacteria. Infection occurs from a patient through airborne droplets during talking, coughing and sneezing. Purulent inflammation of the membrane of the brain and its parts occurs.
- Alcohol
has a very strong effect on certain parts of the nervous system, including the cerebral cortex. At the stage of mild intoxication, the processes of inhibition of the nervous system are weakened, the speech zones of the cortex are excited, speech becomes loud, incoherent, and attention is easily distracted. With moderate intoxication, inhibition of subcortical zones is weakened. IVAN Petrovich PAVLOV called the excited state of these zones “a rebellion of the subcortex.” Not only insults to others begin, but also fights. When the visual cortex is disrupted, the vision begins to double.
Poem
:
The damned villain dried me up, I have no more bright ideas, He stole my neurons and exchanged them for a pack of cigarettes. Now and for a long time I cannot learn this lesson, I have no attention and no memory - All from these damned cigarettes. A strict sentence: for the passion for smoking, the room of the mind becomes empty, Where there was a world of ideas, now there is darkness. [1]
Conclusion
: The cerebral cortex is the highest department of the central nervous system, responsible for mental and speech activity, memory, and the functioning of the sensory organs, muscles and joints. The cerebral cortex is the “master computer of the body”
IV. Homework
(9–10, report on the effects of drugs on the nervous system.)
Lesson grades.
V. Lesson summary
(Cards are given to 2 students - read aloud.)
Cards 2
- In 1 cubic mm of the cerebral cortex contains at least 30,000 neurons. The brain reacts to only 1% of information; 99% of information is “discarded” as unnecessary.
- One of Franz Gahl's students performed 700 brain autopsies and confirmed that speech disorders are associated with diseases of the frontal lobe of the cerebral cortex.
- Smoking is one of the causes of various nervous disorders in adolescents. They sleep poorly, become irritable, absent-minded, memory and attention weaken, and brain function slows down. [2]
- Bad habits need to be banished, and a healthy lifestyle is necessary for everyone.
- I.P. Pavlov said: “...the progress of natural science, unstoppable since the time of Galileo, for the first time noticeably stopped in front of the higher part of the brain.”
Card 1
- Nervous regulation of physiological processes consists in the interaction of body organs with the help of ____________________
- The nervous system is divided into two parts: __________________________
- Clusters of neuron cell bodies form the ___________________________ of the brain and spinal cord.
- The bodies of nerve cells can also lie outside the central nervous system, near internal organs or in their walls, forming here ________________________
- An electrical wave traveling along a nerve fiber is called _______________________
- The body's response to irritation of sensitive formations - receptors, carried out with the participation of the nervous system is ___________________
- The forebrain consists of the diencephalon and ____________________________
Brain disorders
Unlike epileptic conditions, which are caused by dysfunction of the right temporal lobe of the brain, the feelings of an ordinary person manifest themselves systematically, and not in fits and starts.
As a result of voluntary subjects, it was revealed that forced activation of the temporal lobes of the brain is felt by a person as supernatural experiences, sensations of the presence of a non-existent object, angels, aliens, and a feeling of transition beyond the limits of life and approaching death was also recorded.
Awareness of a double or “other self” arises due to a mismatch between the hemispheres of the brain, according to experts. If emotional perception is stimulated, extraordinary, so-called spiritual experiences arise.
The passive temporal lobe hides intuition; it is activated when you have the feeling that someone you know is not feeling well, although you cannot see them.
Among patients suffering from an illness of the medial areas of the temporal lobe, there were cases of extreme emotionality, as a result of which highly ethical behavioral manifestations developed. The behavior of patients with hyperactive gyri of the temporal lobe was monitored by rapid and coherent speaking, and at the same time, a relative decrease in sexual activity was noticeable. Unlike other patients with a similar type of disease, these patients showed signs of depression and bouts of irritability, which contrasted with their friendly attitude towards themselves.
Speech motor area
Allows you to ensure the normal functioning of the facial muscles, which is necessary for pronouncing complex phrases and words. To put it differently, thanks to the speech motor area, speech is formed in a person as a whole. If he is right-handed, then in the left hemisphere the speech motor zone takes up much more space than in the right, and if he is left-handed, everything is exactly the opposite.
If the zone is destroyed or severely damaged, the ability to speak is automatically lost. In this case, a person will be able to sing and scream without words. Also, if damaged, the ability to read to oneself and formulate one’s thoughts is lost. Such damage does not affect the function of understanding the speech of other people.