Content
- 1 General information
- 2 Pharmacological action
- 3 Pharmacokinetics
- 4 Indications
- 5 Contraindications 5.1 With caution
- 8.1 From the digestive system
general information
Dihydroxyphenylalanine (DOPA, dopa, dopa) is a biogenic substance formed in the body from tyrosine and is a precursor to dopamine, which in turn is a precursor to norepinephrine.
Due to the fact that in parkinsonism the content of dopamine in the basal ganglia of the brain is reduced, for the treatment of this disease it is advisable to use substances that increase the content of this amine in the central nervous system. Dopamine itself cannot be used for this purpose, since it does not penetrate the blood-brain barrier well. It turned out that instead of dopamine, its precursor, dioxyphenylalanine (dopa), can be used, which, when administered orally, is absorbed, penetrates the central nervous system, undergoes decarboxylation, turns into dopamine and, replenishing its reserves in the basal ganglia, stimulates dopamine receptors and provides a therapeutic effect for parkinsonism .
The drug used is a synthetic levorotatory isomer of dioxyphenylalanine - L-dopa, which is much more active than the dextrorotatory isomer.
pharmachologic effect
Eliminates hypokinesia, rigidity, tremor, dysphagia, salivation. Most is converted to dopamine in peripheral tissues; The dopamine formed here is not involved in the implementation of the antiparkinsonian effect of levodopa (does not penetrate the central nervous system) and is responsible for most of its side effects. In this regard, it is advisable to combine levodopa with peripheral dopa decarboxylase inhibitors (carbidopa, benserazide), which can significantly reduce the dose of levodopa and the severity of side effects. To reduce decarboxylation, levodopa is used with dopa decarboxylase inhibitors (see Nakom, Madopar). The therapeutic effect is observed after 6-8 days, and the maximum effect occurs after 25-30 days. It has been established that the therapeutic effect is achieved in 50-60% of patients. For the rest, the effect is mild; the dose of the drug cannot be increased due to side effects.
Pharmacokinetics
When taken orally, it is quickly absorbed from the gastrointestinal tract, absorption is 20-30% of the dose (depending on the rate of evacuation of the contents of the stomach and the contents in it). The presence of food in the stomach slows down absorption. Some dietary amino acids may compete with levodopa for absorption from the intestine and transport across the BBB. When taken orally, TCmax is 1-2 hours. Large quantities are determined in the small intestine, liver and kidneys, only about 1-3% penetrates the brain. Metabolized in all tissues, mainly by decarboxylation to form dopamine, which does not penetrate the BBB. T1/2 - 3 hours. Excreted by the kidneys in the form of metabolites (dopamine, norepinephrine, epinephrine) - about 75% within 8 hours, through the intestines - 35% within 7 hours.
Pharmacological properties of the drug Levocom
Pharmacodynamics . Levocom is a combined antiparkinsonian drug that contains levodopa, a metabolic precursor of dopamine, which, unlike the latter, passes through the BBB, and carbidopa, an inhibitor of aromatic amino acid decarboxylase. Due to decarboxylation, levodopa is converted into dopamine in brain tissue, replenishing its deficiency and thereby reducing the severity of parkinsonism symptoms. Levodopa reduces the severity of many symptoms of the disease, especially rigidity and bradykinesia. Reduces tremor, dysphagia, sialorrhea, orthostatic instability associated with Parkinson's disease and syndrome. However, a significant portion of ingested levodopa is converted to dopamine outside the brain and does not cross the BBB. Carbidopa, which does not cross the BBB, interferes with the extracerebral decarboxylation of levodopa, thereby increasing the amount of levodopa that enters the brain and is converted there to dopamine. The advantages of the combination drug are better therapeutic effect and patient susceptibility compared to levodopa; less pronounced side effects, since lower doses of levodopa are used to achieve a therapeutic effect. The drug effectively provides prolonged levels of levodopa in the blood plasma. Carbidopa interferes with the action of pyridoxine hydrochloride (vitamin B6), which accelerates the peripheral metabolism of levodopa. Pharmacokinetics. The active components that make up the drug undergo a number of transformations. Levodopa is well absorbed from the gastrointestinal tract, mainly in the small intestine. Distributed between organs and tissues. Levodopa undergoes complex metabolic transformations, the main of which is its decarboxylation with the formation of dopamine, norepinephrine and adrenaline, which are secreted by the kidneys. About 80% of levodopa is excreted in the urine, mainly in the form of dihydroxyphenylacetic acid and homovanillic acid. Less than 1% is excreted unchanged. The half-life of levodopa from blood plasma is about 1 hour; in the presence of carbidopa, the half-life increases to 2 hours. Carbidopa (alpha-methyldopahydrazine) after oral administration is quickly but not completely absorbed into the gastrointestinal tract. Distributed in the body, does not penetrate the BBB. About 50% is excreted unchanged and in the form of metabolites by the kidneys. Levokom retard. Levocom retard is a combination of the decarboxylase inhibitor carbidopa and the metabolic mediator dopamine levodopa in the form of long-acting polymer-based tablets. Levocom retard is especially indicated for reducing the period of retardation in patients who were previously treated with the usual combination of levodopa with a decarboxylase inhibitor and who have manifestations of dyskinesia and motor fluctuations. Absorption of levodopa after the use of levodopa/carbidopa 200/50 mg with slow release lasts more than 4-6 hours. Due to this, fluctuations in the concentration of levodopa in the blood plasma are observed within a narrower range than with the use of levodopa/carbidopa tablets with immediate release. The bioavailability of levodopa from extended-release tablets (containing levodopa/carbidopa) is approximately 70% compared to immediate-release tablets. Therefore, the daily dose of levodopa in extended-release levodopa/carbidopa tablets should be higher than in immediate-release tablets. The average time to reach maximum plasma concentrations for extended-release tablets 200/50 mg is about 2 hours. Food intake does not affect the absorption of levodopa, but reduces the bioavailability of carbidopa by 50% and the maximum plasma concentration by 40%. However, a decrease in the level of carbidopa in the blood plasma has no clinical significance. In the presence of carbidopa, levodopa is metabolized to amino acids and, to a lesser extent, to catecholamine derivatives. All metabolites are excreted by the kidneys.
Contraindications
Contraindicated in cases of severe atherosclerosis, hypertension with a significant increase in blood pressure, with uncompensated endocrine, renal, hepatic, cardiovascular, pulmonary diseases, narrow-angle glaucoma (with wide-angle glaucoma, treatment is carried out under careful monitoring of intraocular pressure and with ongoing antiglaucomatous therapy), with diseases blood, melanoma, as well as in case of individual hypersensitivity to the drug. Levodopa and drugs containing levodopa are not recommended for pregnant women, nursing mothers and children under 12 years of age.
Carefully
Levodopa should be prescribed to patients with bronchial asthma, emphysema, patients with active gastric ulcers, psychoses and psychoneuroses, and patients who have suffered a myocardial infarction in the past.
Special instructions for the use of Levocom
Levocom is not used to eliminate extrapyramidal reactions caused by drugs. The drug is indicated for patients with parkinsonism who are taking vitamin preparations containing pyridoxine hydrochloride (vitamin B6). All patients taking the drug should be closely monitored to identify mental changes and depressive syndrome. Patients with psychosis (including a history) require special medical supervision during treatment. The drug should be prescribed with caution to patients with cardiovascular diseases, severe pulmonary diseases, asthma, diabetes mellitus, mental disorders, seizure syndrome, open-angle glaucoma, a history of peptic ulcers of the stomach and/or duodenum (due to the possibility of bleeding from the upper gastrointestinal tract ), for diseases of the kidneys, liver and endocrine system organs. It is also prescribed with caution to patients who have recently suffered a myocardial infarction in the presence of ventricular arrhythmia. Such patients are advised to monitor the state of the cardiovascular system, especially while determining the initial dose. Patients who develop choreoathetoid-type hyperkinesis while taking the drug should be monitored. Levocom in some cases can cause a relapse of hyperkinesis, which may be a consequence of an increase in the level of dopamine in the brain, in which case it is necessary to reduce the dose of the drug. If it is necessary to prescribe psychotropic drugs, one must take into account the possibility of reducing the antiparkinsonian effect of Levocom. In patients with chronic open-angle glaucoma, systematic ophthalmological monitoring is required when taking the drug. If it is necessary to perform an operation under anesthesia, Levocom is discontinued the day before and resumed after the operation as soon as the patient is able to take the drug orally. If the drug is discontinued, the dose is reduced gradually, and the patient's condition must be carefully monitored. During the period of use of the drug, it is necessary to regularly monitor the functional state of the liver, kidneys, cardiovascular system and hematopoietic system. Levodopa preparations with carbidopa can cause a false-positive reaction for the presence of ketone bodies in the urine, as well as deviations in the results of various laboratory parameters - liver tests, alkaline phosphatase, ALT, AST, LDH, bilirubin, in the test for the presence of blood in the urine and the Coombs reaction. False-positive results can be obtained when using the glucose oxidase method for determining glycosuria. During pregnancy and breastfeeding. The drug is contraindicated during pregnancy and breastfeeding. To prevent the occurrence of negative reactions in children, a decision must be made either to stop breastfeeding or to stop taking the drug, taking into account the need for the mother to take it. Children. Not used. The ability to influence reaction speed when driving vehicles and other mechanisms. Some side effects (dizziness, drowsiness, dyskinesias) observed during treatment with Levocom affect the ability to drive vehicles or operate machinery.
Dosage regimen
Inside. Treatment begins with small doses, gradually increasing them to the optimal dose for each patient. The initial dose is 0.25-1 g in 2-3 doses. The dose is gradually increased by 0.125-0.75 g every 2-3 days, depending on tolerability and until the optimal therapeutic effect is achieved. The maximum daily dose is 8 g. Cancellation is carried out gradually. The drug is taken with food or with a small amount of liquid; the capsules are swallowed whole. To obtain the best therapeutic effect with the least side effects, the dose of the drug should be selected individually, starting with a relatively small dose and gradually increasing it. It is necessary to carefully monitor the patient's condition, especially at the beginning of treatment. Levodopa can be prescribed simultaneously with anticholinergic drugs. The combined use of anticholinergics with levodopa is effective for rigid-bradykinetic and tremulous forms of vascular parkinsonism. You can also combine the use of levodopa and midantan.
Use of the drug Levocom
In adults inside. Levokom. The optimal daily dose of the drug must be carefully selected for each patient. For patients starting treatment with the drug, the initial dose is tablets 1-2 times a day after meals. If necessary, the dose is increased by gradually adding a tablet daily or every other day until the optimal therapeutic effect is obtained. The maximum daily dose of Levocom tablets is 8 tablets (200 mg of carbidopa and 2 g of levodopa). Levokom retard. Extended-release tablets can be divided, but should not be chewed to preserve the properties of the drug. The optimal daily dose of the drug must be carefully selected for each patient. During the dose selection process, the patient should be constantly monitored, especially if side effects such as nausea and pathological involuntary movements, in particular dyskinesia, chorea or dystonia, occur or worsen. An early manifestation of an overdose may be blepharospasm. Patients who have not previously taken levodopa drugs. The recommended starting dose is 1 extended-release tablet 2-3 times daily and should not exceed 3 tablets (600 mg levodopa) per day. There should be an interval of at least 6 hours between individual doses. The dose is selected at intervals of at least 2–4 days. Depending on the severity of the disease, the optimal therapeutic effect can be achieved within 6 months of treatment. Dosage recommendations for patients receiving levodopa formulations with an immediate-release decarboxylase inhibitor. At least 12 hours should elapse between the last dose of levodopa + decarboxylase inhibitor and the first dose of Levocom retard. The transition to taking Levocom retard should occur when prescribed in doses that allow increasing the daily dose of levodopa by no more than 10%, although it may be necessary to exceed the daily dose levodopa dose compared to previous therapy by 30%. The interval between individual doses should be increased to 4–12 hours. If the daily dose is divided into unequal single doses, it is recommended to take the minimum single dose at the end of the day. Recommendations for switching from taking immediate-release levodopa/carbidopa tablets to extended-release Levocom retard tablets are given in the table.
Levodopa/Carbidopa Rapid Release Tablets | Levocom retard 200/50 mg, extended-release tablets | |
Daily dose of levodopa, mg | Daily dose of levodopa, mg | Number of extended-release tablets per day |
| 100–200 | 200 | Tablets 2 times a day |
| 300–400 | 400 | 1 tablet 2 times a day |
| 500–600 | 600 | 1 tablet 3 times a day |
| 700–800 | 800 | 4 tablets in 3 or more divided doses |
| 900–1000 | 1000 | 5 tablets in 3 or more doses |
| 1100–1200 | 1200 | 6 tablets in 3 or more doses |
| 1300–1400 | 1400 | 7 tablets in 3 or more doses |
| 1500–1600 | 1600 | 8 tablets in 3 or more doses |
Patients receiving levodopa monotherapy (without a decarboxylase inhibitor). At least 12 hours must pass between the last dose of levodopa and the first dose of Levocom retard. In patients with mild to moderate disease, the recommended initial dose is 1 tablet (200/50 mg) 2 times a day. Dose selection. Once the drug regimen has been determined, the dose or frequency of administration may be increased depending on the patient's response. The dose is adjusted by increasing the daily dose of Levocom retard tablets every 2–3 days until the optimal effect is achieved. Compared to immediate-release levodopa/carbidopa tablets, the effect of the first dose taken in the morning may be delayed by up to an hour in some patients. Maintenance dose . Because the manifestations of Parkinson's disease may change during treatment, regular routine assessment of patients is recommended. In this case, it may be necessary to adjust the dose of the drug.
special instructions
When you stop taking levodopa, the symptoms of parkinsonism usually resume, and if the drug is quickly discontinued after long-term therapy, the symptoms of the disease can sharply increase. It was previously stated that the use of levodopa is contraindicated with the simultaneous administration of monoamine oxidase inhibitors (MAOIs). This position is currently being clarified. The drug should not be used in combination with irreversible MAO type A inhibitors (see Nialamid). In case of previous prescription of irreversible MAO inhibitors, their use should be discontinued at least 14 days before starting levodopa. However, MAO type B inhibitors have recently been proposed to enhance the effect of levodopa (see Deprenyl). If general anesthesia is necessary, you should stop taking levodopa 24 hours before. During treatment, it is necessary to periodically conduct blood tests and check liver and kidney function. In case of severe side effects, it is necessary to stop taking the drug.
Levocom overdose, symptoms and treatment
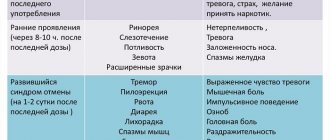
Symptoms : early signs - muscle twitching, blepharospasm; AH (arterial hypertension), increased heart rate, decreased appetite; confusion, agitation, insomnia, restlessness. Treatment : artificially induce vomiting, urgently rinse the stomach. Symptomatic therapy: infusions are prescribed with caution, paying attention to the patency of the airways; When arrhythmia occurs, appropriate treatment is used under ECG monitoring. The value of dialysis for the treatment of overdose events has not been studied. The use of pyridoxine hydrochloride is ineffective.
Side effects
From the digestive system
Decreased appetite, nausea, vomiting, constipation, dysphagia, ulceration of the gastrointestinal mucosa, gastralgia, gastrointestinal bleeding (in patients with a history of peptic ulcer).
From the nervous system
Drowsiness or insomnia, anxiety, dizziness, paranoid states, hypomania (with increased sexual desire and antisocial behavior), euphoria, depression, dementia, ataxia, convulsions, spasmodic torticollis, dyskinesia, choreiform, dystonic and other uncontrolled movements, suicidal thoughts.
From the cardiovascular system
Decreased blood pressure, orthostatic collapse, arrhythmias, tachycardia.
From the hematopoietic organs
Leukopenia, thrombocytopenia.
Others
Polyuria; rarely - diplopia.
Interaction
With simultaneous use of levodopa with beta-agonists, ditilin and drugs for inhalation anesthesia, the risk of developing heart rhythm disturbances may increase; with tricyclic antidepressants - decreased bioavailability of levodopa. With diazepam, clozepine, phenytoin, clonidine, m-cholinergic blockers, antipsychotic drugs (neuroleptics) - derivatives of butyrophenone, diphenylbutylpiperidine, thioxanthene, phenothiazine; pyridoxine, papaverine and reserpine may reduce the antiparkinsonian effect. With Li+ drugs, the risk of developing dyskinesias and hallucinations increases; with methyldopa - worsening side effects. When levodopa is used simultaneously with MAO inhibitors (except for MAO-B inhibitors), circulatory disorders are possible (taking MAO inhibitors should be discontinued 2 weeks before). This is due to the accumulation of dopamine and norepinephrine under the influence of levodopa, the inactivation of which is inhibited by MAO inhibitors, and a high likelihood of developing agitation, increased blood pressure, tachycardia, facial flushing and dizziness. In patients receiving levodopa, the risk of a significant decrease in blood pressure increases when using tubocurarine.
Drug interactions Levocom
You should be careful when using Levocom simultaneously with such drugs. Antihypertensive drugs . When using levodopa/carbidopa with some antihypertensive drugs, the development of symptomatic orthostatic disorders is possible, therefore, in the process of selecting the dose of Levocom, dose adjustment of concomitant antihypertensive drugs is necessary. Antidepressants. Occasionally, with the simultaneous use of levodopa/carbidopa and tricyclic antidepressants, side effects may occur in the form of hypertension (arterial hypertension) and dyskinesia. Anticholinergics . Levocom can be used with anticholinergics that have a synergistic effect with levodopa in reducing tremor. However, their general use may increase involuntary movement disorders. Anticholinergics may enhance the effects of levodopa due to delayed absorption. In such cases, dose adjustment of levodopa/carbidopa is necessary. Other antiparkinsonian drugs . Anticholinergics, dopamine antagonists, and amantadine can be used with Levocom. Moreover, if these drugs are prescribed in addition to therapy carried out by Levocom, it may be necessary to adjust the doses of these drugs. The general use of selegeline with levodopa/carbidopa can provoke severe orthostatic disorders. Other medicines . Since carbidopa prevents the reduction in the effects of levodopa caused by the use of pyridoxine (vitamin B6), Levocom can be used in patients who are additionally receiving pyridoxine. The drug should not be taken simultaneously with MAO inhibitors. These drugs must be discontinued 2 weeks before taking Levocom. Dopamine D2 receptor antagonists (eg phenothiazines, butyrophenones, risperidone), benzodiazepines and antituberculosis drugs may reduce the therapeutic effect of levodopa. The beneficial effects of levodopa in Parkinson's disease may be reduced when used concomitantly with phenytoin and papaverine. In these cases, careful monitoring by a doctor is required due to the possibility of reducing the effectiveness of treatment. The general use of catecholomethyltransferase inhibitors (tolcapone, entacapone) and levodopa/carbidopa may increase the bioavailability of carbidopa. Amantadine exhibits synergistic effects with levodopa and may increase the side effects of levodopa. In this regard, dose adjustment of levodopa/carbidopa may be necessary. Metoclopramide accelerates gastric emptying and may increase the bioavailability of Levocom. Sympathomimetics may potentiate the cardiovascular side effects of levodopa. The use of ferrous sulfate and levodopa/carbidopa may reduce the absorption of levodopa. Because levodopa competes with certain amino acids, absorption of levodopa may be impaired in some patients on a protein-rich diet.