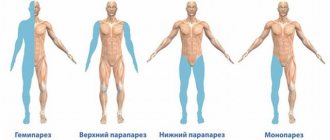
Forms, types and classifications of apraxia
- Kinesthetic: it is impossible to control one’s own movements, for example, to tie one’s shoelaces and fasten buttons on one’s own, and also to show an action without the object itself that is necessary for this, for example, to show how to turn on the water.
- Kinetic or dynamic: it is impossible to build the correct sequence of actions, since the transition from one separate simple movement to another is disrupted.
- Regulatory: the ability to perform unusual, new and not necessarily complex manipulations is impaired, so the patient uses familiar patterns, for example, trying to put out a lighter like a match.
- Spatial and constructive: the ability to create a whole from several parts, to compare concepts “top-bottom”, “left-right”, etc. is impaired, so the patient cannot get dressed, make the bed or perform other simple tasks.
There is no unified classification of the disease, since its nature has not yet been fully studied by specialists. Some doctors distinguish types of apraxia depending on the disorders themselves (motor apraxia, speech apraxia, etc.), on the part of the brain responsible for motor activity (frontal, cortical, etc.), on the side of the body (unilateral and bilateral), etc. Also There are ideomotor apraxia, in which it is impossible to perform even simple movements, ideational, in which it is impossible to perform a chain of complex actions, despite the fact that the patient performs individual actions quite easily, limbic-kinetic, in which the accuracy and dexterity of movements (usually the fingers) are impaired.
Etiology, risk factors
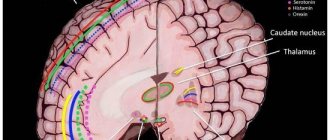
Manifestations of apraxia are associated with damage to the parietal, frontal lobes of the cerebral cortex, and corpus callosum. The following pathologies can provoke this condition:
- dementia arising from chronic lack of blood circulation;
- traumatic brain injuries;
- encephalitis;
- Alzheimer's disease;
- brain tumors;
- Parkinson's disease.
If you have one of the diseases described above, you need to regularly monitor your health over time.
Symptoms of apraxia
Patients cannot perform various actions, while the sensitivity of the limbs and muscle tone are not impaired - the person remains physically healthy.
As a rule, people with a similar diagnosis cannot move from one movement to another or repeat a certain pose. For example, if the patient does not see and does not hold a cup, then he cannot show how to hold it; if he fastens buttons on clothes, then he cannot understand what movements with his fingers need to be made; if a person is used to using a lighter, then he will try to light a candle with a match. on the same principle.
With significant impairments, patients not only cannot perform purposeful actions, but also completely lose the ability to independently care for themselves.
Types of motor apraxia
With motor apraxia, both spontaneous actions and imitation actions occur. This type of disease is most often unilateral. Motor apraxia is divided into two types - melokinetic and ideokinetic. With ideokinetic apraxia, the patient is not able to consciously perform simple movements, but can perform them accidentally. He performs simple actions correctly, but not according to instructions. The patient usually confuses movements (touches his nose instead of his ear, etc.). Melokinetic apraxia manifests itself in a distortion of the structure of movements that make up a specific action and their replacement with vague movements in the form of moving and spreading fingers instead of clenching the hand into a fist or shaking a finger.
Benefits of rehabilitation in
Extensive experience and attentiveness allow our specialists to find an approach to patients and select optimal rehabilitation methods in a particular case. We believe that there can be no trifles in medicine: our center employs only competent, qualified specialists (from administration staff and nurses to doctors), we use new, modern and at the same time proven effective equipment and techniques, we adhere to an individual and multidisciplinary approach, our psychologists and psychotherapists are always ready to help patients cope with depression and accept new living conditions. We also thought through the architecture of the center: wide doorways, threshold-free anti-slip coating, ramps and handrails are especially important for people with disabilities.
We want your well-being to not depend on circumstances!
Principles of treatment
For therapy to be successful, classes should take place up to 3-5 times a week. Individual lessons are preferable to group exercises, especially at the initial stage. Subsequently, subject to positive dynamics, tactics can be changed. Parents of a child with apraxia must be patient and actively participate in the development program. A favorable family environment facilitates the treatment process.
Therapy for apraxia should begin with eliminating the cause of the pathology, that is, treating the underlying disease.
In addition to taking medications according to an individual regimen for each patient, physiotherapeutic methods help improve the quality of life. If we are talking about the oral form, classes with a speech therapist are necessary. The prognosis is favorable, of course, subject to systematic treatment and exercise. Close relatives should be patient with the manifestations of the disease and the patient’s lifestyle, and help him in everyday life.
There are no special recommendations for preventing the disease. They are common. This includes a healthy lifestyle, a balanced and rational diet, and timely examination by a doctor in the presence of complaints and chronic infections. In case of health problems due to vascular problems, it is necessary to monitor blood pressure levels.
What is apraxia
Every day a person has to perform a huge number of actions - simple, complex, compound. We perform some of these actions automatically, without thinking about them at all. The other part of the action requires a clear and thoughtful plan.
The ancient Greeks called the ability for purposeful movements the word “praxis,” which has survived to this day. Therefore, apraxia
is the loss of the ability to perform such actions.
Performing successive sets of movements is the highest mental function acquired by man in the process of long evolution. This function is acquired by a person only in the process of life - through learning and the accumulation of some individual experience. Certain disorders in the functioning of the brain lead to the loss of this function. A person can perform simple actions that are components of a complex complex, but combining them into this same complex becomes problematic for him.
Despite the fact that human “praxis” has been studied by scientists and philosophers for thousands of years, specialists’ attention to apraxia appeared only in the second half of the nineteenth century, when this term appeared. In 1871, the concept of “apraxia” was first used by the German philologist Heymann Steinthal; however, a detailed description of the symptoms of this disease was presented much later - this was done already in the twentieth century by the German doctor G. Lielmann.
Symptoms
The difficulty in establishing the disease is that symptoms may not indicate the development of pathology for a long time. In some cases, they are not pronounced and cause slight discomfort to the person. Most often, the presence of a problem is determined during an examination by a neurologist.
Apraxia may have symptoms such as:
- A person has difficulty performing actions consistently.
- Difficulty in reproducing actions that require orientation in space.
- Slurred speech.
- Walking in small steps. Often a person walks very hunched over, shuffles his feet, and when an obstacle arises in front of him, he thinks for a long time about how to overcome it.
- Difficulties arise with the process of dressing.
- It is difficult for a person to open or close his eyes.
- Impaired spatial orientation.
- Inability to fixate the gaze on an object.
- A person cannot control the movement of his tongue and lips.
In addition to these manifestations of pathology, a person is worried about aggressiveness, irritability, and a tendency to depression.
Standard Treatments
When apraxia is a symptom of an underlying disorder, the disease or condition must be treated. Physical and occupational therapy may be helpful for patients with stroke and head injury. When apraxia is a symptom of another neurological disorder, the underlying condition must be treated. In some cases, children with apraxia can learn to compensate for deficits as they grow older through special education programs and physical therapy.
Speech therapy and special education may be especially helpful in treating patients with developmental apraxia of speech.
Signs and symptoms
The main symptom of apraxia is the inability of a person to perform movements in the absence of any physical paralysis. The commands to move are clear, but cannot be executed. When the movement begins, it is usually very clumsy, uncontrollable and inappropriate. In some cases, movement may occur unintentionally. Apraxia is sometimes accompanied by a person's loss of ability to understand or use words (aphasia).
Certain types of apraxia are characterized by the inability to perform certain movements on command. For example, with apraxia of the cervicofacial region, a sick person cannot cough, whistle, lick his lips or wink when asked to do so. With the constructional type of the disease, a person cannot reproduce simple patterns or copy simple drawings.
Treatment of apraxia in Saratov, Russia, therapy of apraxia
Sarklinik provides treatment for certain types of apraxia in adults, adolescents, children, boys, girls, boys, girls, men, women in Saratov, Russia. The doctor knows how to treat apraxia , how to cure apraxia, how to get rid of apraxia, what to do with apraxia, where to go. At the first consultation, will the doctor tell you what types of apraxia there are? What are the characteristics of kinesthetic (kinetic) apraxia, aphasia and agnosia ? Why does oral apraxia, motor apraxia, constructive apraxia, articulatory apraxia, regulatory apraxia occur in children and adults? What is apraxia of walking and speech? What is the danger of motor left, right hand, left, parva leg, fingers, ideator apraxia? What are the principles for diagnosing apraxia ? Unfortunately, traditional methods, traditional medicine, diet, pills, medicines, drugs, traditional methods, spells, homeopathy rarely help in the treatment of apraxia. On the website sarclinic.ru you can see a doctor online for free.
Sign up for a consultation. There are contraindications. Specialist consultation is required.
Related posts:
Where in Saratov you can cure your nerves
Millard–Gubler syndrome (A. Millard, AM Gubler) alternating pontine
Kogan syndrome: treatment, how to treat Kogan, oculomotor apraxia
Causes of urinary incontinence in women and men, treatment in Saratov
Weber's syndrome HD Weber, alternating peduncular syndrome
Comments ()
Causes and possible diseases
Apraxia is caused by brain damage (brain damage) in the vocal dominant hemisphere. This is usually a left-sided (or bilateral) stroke or other lesion. In addition, apraxia can also be caused by, for example, degenerative diseases. For example, Alzheimer's disease is the most common cause of severe apraxia. Other forms of dementia (dementia with Lewy bodies, frontotemporal dementia = Pick's disease) can also cause this disorder.
User reviews about the help of CF in the treatment of apraxia
Apraxia Article #1
Apraxia.
Classification A.R. Luria A disorder of motor skills, a violation of purposeful actions, causes the disease “apraxia”.
In order to use motor skills, a certain movement pattern, formed in advance, is required. Patterns are remembered and reproduced automatically when circumstances require it.
There are several stages that make up any activity. The urge to act, which arises in certain situations, is the first of these. The left parietal-temporal region is connected to the left premotor zone, which controls all movements of the right hand, and through it has connections with the right hemisphere and its motor zone, the task of which is to control the left limbs. Therefore, damage to the midline parts of the corpus callosum causes apraxia in the left extremities, but if the damage occurs in the left parietal-temporal region, total apraxia will develop.
Apraxia can be identified by looking at how the patient performs any actions, for example, how he uses a comb or toothbrush, whether he is able to repeat his gestures after the doctor, or perform tasks related to words.
Several forms of impaired actions are combined under the name “apraxia”.
A.R. Luria and G. Lipman proposed their classifications of the disease.
A.R. Luria is a Russian neuropsychologist who has written works that have become especially significant for the study of apraxia and other disorders. In 1947, in his classification of apraxia, he identified four forms based on the psychological structure and brain organization of motor actions.
- Apractoagnosia (spatial);
- Afferent (kinesthetic);
- Efferent (kinetic);
- Prefrontal (regulatory).
Damage to the parieto-occipital cortex (especially the left hemisphere) causes spatial apraxia .
At the junction of the temporal, parietal and occipital lobes there is a zone of the statokinesthetic analyzer. Spatial relationships during the performance of motor functions are disrupted when this zone is damaged. Violation of visual-spatial synthesis, as well as spatial representations, underlies spatial apraxia. Thus, in those who suffer from this disease, the visuospatial afferentation of movement is impaired, that is, the impulse that is necessary to perform certain actions does not occur.
Despite the fact that with spatial apraxia, visual gnostic functions are preserved, in most cases it occurs in parallel with visual optical-spatial agnosia (various types of perception are impaired). In all cases, postural apraxia can be observed, and difficulties arise when trying to perform spatially oriented movements. Increased visual control over your movements turns out to be useless. There is no difference when performing motor actions with eyes closed or open.
Constructive praxis
(the ability to perform purposeful movements) also refers to this type of disorder. Difficulties arise when drawing and constructing any figures from parts.
Patients are unable to draw or copy geometric shapes, images of animals, objects from memory. The contours of the drawn object are distorted (instead of an oval there is a circle), some individual elements and details are not drawn (one corner of the square remains undrawn, for example). It is quite difficult to copy complex shapes, such as a rhombus, a five-pointed star (instead of a star, an irregularly shaped triangle). Copying irregular geometric figures turns out to be almost impossible for patients with apraxia.
Trying to draw a human or animal figure also causes great difficulties. The contours of a person are not fully drawn, the elements are disproportionate and distorted. If the patient draws a human face, then the ear may be inside the face, one eye above the other.
The patient is unable to draw from memory. Difficulties arise when drawing three-dimensional three-dimensional images (pyramids, cubes). If the patient depicts a table, then all four legs may be on the same plane. Constructing figures from matches or cubes turns out to be almost impossible.
When copying unfamiliar figures that do not have a verbal designation, the disorder of constructive praxis is especially clearly manifested. This technique is often used to diagnose hidden disorders.
Constructive apraxia is caused by difficulty in choosing a place to draw on a piece of paper. The picture can be drawn either in the lower right or upper left corner. A “switch-on symptom” is observed, and the patient begins to draw, leaning close to the sample or by superimposing his own drawing on the sample. In most cases, the left spatial field is ignored when the right hemisphere is damaged.
Constructive apraxia occurs as a result of a lesion in the left (right) hemisphere of the parietal zone. In right-handed people, this defect of higher mental function especially often occurs and is expressed to a more severe degree if a left-sided lesion occurs.
If the left hemisphere is affected, then patients tend to copy samples rather than draw from memory; the drawings are primitive with a small number of details; Difficulties arise when selecting corners. Many elements inherent in this disorder can be identified if one begins to analyze the letter and the construction of numbers and letters in it.
If the parietal lobe near the postcentral gyrus (the lower section near the postcentral region of the cerebral cortex) is affected, then kinesthetic apraxia occurs. If there is a disruption in the left hemisphere, apraxia is bilateral, but if one right hemisphere is affected, then one left hand suffers.
External spatial ability to move is preserved, but proprioceptive kinesthetic afferentation of movements is impaired. Therefore, the disease is also called afferent apraxia. A syndrome called “shovel hand” occurs, in which all motor acts are of an undifferentiated nature, writing movements are impaired, and the patient is unable to correctly copy various hand postures (postural apraxia).
The patient is not able to show how soup is poured into a plate if this action is required to be performed without objects. To some extent, movements can be compensated by strengthening visual control of movements.
Kinetic apraxia is a condition that affects the lower parts of the premotor region in the cerebral cortex. This apraxia
proceeds in parallel with the disturbed temporary organization (automation) of many mental functions.
When the disease occurs, the “kinetic melodies” begin to disintegrate, and the temporal organization and sequence of motor acts are disrupted. In this case, elementary movements (according to Luria) begin to continue following the once started movement and are uncontrolled. Various motor actions are impaired - the ability to draw, write, perform graphic tests, which is especially noticeable if a series of actions occurs. This causes kinetic apraxia.
During prefrontal (regulatory) apraxia, the lesion is located anterior to the premotor regions at the site of the convexital prefrontal cortex. During the disease, muscle strength and tone are preserved.
The disease occurs when the ability to voluntarily control actions is impaired, and speech regulation during motor acts also suffers. Kinetic apraxia is caused by impaired programming of movements, disabling conscious control over them. The necessary actions are replaced by motor stereotypes and patterns. Systemic perseverations (persistent reproduction of the same actions) and perseverations of certain motor programs often occur. Patients find it very difficult to change their usual program of actions and movements.
In certain cases, patients may experience echopraxia syndrome, which is expressed by imitative repetitions of the actions of the person conducting the experiment. This occurs if there is a gross breakdown of voluntary control of actions. If the left prefrontal region of the brain is affected, then this prefrontal apraxia manifests itself most clearly.
Apraxia. Classification according to G. Lipman
According to G. Limpan, there are several types of apraxia: kinetic, ideomotor, ideational, oral, apraxia
body and dressing.
In addition, there is also agraphia, which is caused by a writing disorder.
- With kinetic apraxia of the limbs, the patient retains muscle strength, active movement, he can take care of himself, but difficulties arise when performing ordinary gestures and actions (move the hand or fingers).
The pattern according to which certain gestures are performed is preserved, and the ability to reproduce elementary actions and gestures, which are based on certain symbolism, is impaired. Let’s say “wave goodbye”, “beckon with your finger”. - With ideomotor apraxia the ability to perform intentional actions, for example, actions on command, is impaired, although they are spontaneously performed correctly. The patient loses the ability to implement the necessary actions, although he can describe the actions given according to the command. Let's say he won't be able to show his ear or clench his fist if there was a command to perform these actions. Although he will easily perform these actions spontaneously. If there is no object of action, then the task becomes especially difficult to complete. Patients find themselves unable to reproduce the way they cut down a tree, stir soup in a pan, or open a door. Movements are deformed and mixed with movements in other actions.
The patient performs symbolic actions easily. According to many authors who study apraxia, ideomotor bilateral apraxia often occurs if the supramarginal gyrus in the left parietal lobe is affected. Kinetic limb apraxia occurs when areas near the posterior central gyrus are affected.Lesions of the parietal lobe, which include the angular gyrus, cause a combination of ideomotor apraxia and ideational apraxia. These forms of apraxia are rarely found in their “pure” form. With ideomotor apraxia, the right hemisphere and the corpus callosum in the middle sections are affected. If the supramarginal gyrus in the left hemisphere is affected, bilateral apraxia occurs. This form is rare if the right hemisphere is affected. In this case, there is a defect in the left limbs.
- Ideator apraxia in a single form is extremely rare. The patient can perform simple actions, but complex actions that require a certain sequence cause difficulties. If you copy every fragment that is included in the scheme of complex actions, then it is performed correctly. For example, if a patient with ideation apraxia is given a lit match, he will light the candle. But he will not be able to carry out the entire scheme of actions - take a box of matches, pull out one, light, light a candle.
The patient is helpless when performing complex actions. He can twirl the box for a long time, scratch the wrong side of the box with a match, and put the list in his mouth.Simply put, with ideator apraxia
the patient does not know in what sequence to perform the action; with ideomotor apraxia, the patient does not know how to perform the action.
Many doctors believe that ideation apraxia
is always bilateral.
Specialized types of ideation apraxia are oral apraxia , dressing apraxia apraxia . - With oral apraxia, there is a violation of the intentional movements that the lips and tongue make. Patients are unable to reproduce articulatory postures: touching the upper lip with the tongue, sticking out the cheek with the tongue. Symbolic actions performed with the lips and tongue are disrupted. It becomes impossible to click or twirl your tongue, smack your lips, whistle, or show how to spit. Swallowing apraxia is extremely rare. Some doctors classify it as facial apraxia rather than oral apraxia.
Actions that the patient cannot perform according to instructions, he easily performs while eating, while talking and in other everyday situations. This justifies the fact that oral apraxiaclassified as ideomotor.
Symbolic oral apraxia and oral apraxia , separately or together, almost always occur in parallel with motor aphasia (speech impairment). - During apraxia of the trunk, the patient is unable to properly position the lower limbs and trunk in space to sit, stand, or walk. Disorders begin that are designated in the neurological literature by the term “astasia-abasia.” Despite all the disorders, the lower limbs retain their ability to move. This apraxia is localized in the parietal region; in most cases, the connection with the thalamus is disrupted in both hemispheres.
- One of the forms of ideational apraxia , during which the complex pattern of actions when dressing is disrupted, is called apraxia of dressing. Patients are unable to perform the correct sequence of actions that are necessary to undress or dress. They are unable to orient a piece of clothing in relation to a part of the body. Let's say the patient puts his shirt on over his head and puts it through his left sleeve into his right hand, and vice versa, puts it on backwards. Difficulties include putting on shoes, socks, unbuttoning and fastening buttons, and lacing shoes. Apraxia occurs when the angular gyrus (parietal lobe) of the left hemisphere is affected.
Other types of apraxia.
- Frontal apraxia is a variant of motor apraxia. Occurs as a result of impaired ability to perform and program a sequential series of movements. The “kinetic melody”, smoothness and pace of actions are disrupted. There is a tendency to general muscle tension, to repetition of certain elements of movement or motor act (motor perseveration). A person suffering from this apraxia is unable to tap out a certain sequence of weak and strong rhythmic beats; During writing, individual elements of letters or the letters themselves are repeated. Frontal apraxia is caused by damage to the premotor region of the frontal lobe.
- Difficulty placing objects in three-dimensional and two-dimensional space causes constructive apraxia .
A patient with apraxia cannot put several parts together into one whole, for example, the required figure from a mosaic, matches, or cubes. He confuses the directions of movement (goes to the right, if necessary, to the left), confuses the left and right sleeve, left and right shoe, as a result of which he cannot dress himself. The patient is unable to perform these actions, both when commanded and during imitation. Apraxia is caused by the loss of the ability to adequately navigate in space, which occurs due to damage to the cortex of the angular gyrus, the region of the intraparietal sulcus and parts of the occipital lobe. - With gaze apraxia, involuntary actions of the eyeballs are possible, but it becomes impossible to reproduce movements with them. A patient with apraxia cannot turn his gaze on command, but can easily track a moving object with his eyes.
- If apraxia of walking is observed, then walking is impaired, but motor, vestibular, and proprioceptive disorders are absent. This type of apraxia occurs when the frontal cortex (premotor area) is affected.
- When there is a breakdown in the connection between the motor centers and the centers of the sensory component of speech, dissociative apraxia occurs. Independent praxis, as well as repetition of actions after the doctor, is not impaired. The ability to perform movements according to a given command is lost. If the anterior commissure is affected in the corpus callosum, then dissociative apraxia is observed in the left hand. Sometimes there are cases when the apractical disorders described above go in parallel with paresis (partial loss of muscle strength) in the right hand. This set of symptoms is called “sympathetic apraxia.”
- There is also dynamic apraxia, which is caused by damage to deep nonspecific structures of the brain, which causes a violation of involuntary attention. As a result of this factor, automation and assimilation of new patterns of motor acts are difficult for the patient. Errors and failures happen even while executing memorized patterns of action. But in this case, the patient most often pays attention to his mistakes.
Apraxia in children, diagnosis, treatment
Apraxia of speech observed in children is one of the most complex childhood pathologies. Children cannot communicate using words, although their mouth, face, lips and tongue muscles are intact.
Quite often, apraxia of speech occurs as a result of a birth defect. In this case, its identification becomes very difficult, and there is a need for complex diagnostics in a children's clinic. Frequently, children's brains are examined without any abnormalities, although apraxia is thought to result from damage to areas of the brain. Some doctors believe that genetic factors play a major role because, according to statistics, many children's parents (or other family members) suffered from the same disease.
Absolutely all factors and circumstances play a role in violations of a child’s speech development, starting from how he breathes in infancy, how he sucks a breast or bottle, to the moment when it is implied that he should speak.
Many experts believe that spatial apraxia is associated with apraxia of speech. In view of this, the extent to which a child is active in childhood plays a big role both in overall development and in the development of his language skills. In the life activity of many young children there is no movement in the required volume (let's say being in a car for a long time in a static position). From birth, movement deficits may begin.
In many cases, Down syndrome, autism, and congenital diseases that affect muscle tone (cerebral palsy) accompany apraxia of speech. Such children are at risk and have a high probability that they will develop apraxia of speech.
Careful attention must be paid to the treatment of children suffering from apraxia of speech. This disease will not go away on its own, and a child who has not received proper treatment will experience communication difficulties throughout his life.
Infantile apraxia can be treated, but treatment must begin as early as possible. You should contact pediatric speech pathologists who treat children with apraxia of speech. Often a child needs the supervision of such specialists as a neuropsychiatrist, a massage therapist, or a pediatrician. Speech correction is a rather difficult and long process. The child's parents must play a huge role in this process.
The methodology developed by a speech pathologist-defectologist is determined by a specific case. It is compiled after the child’s speech disorder has been carefully studied. Treatment must begin as soon as the parents discover this disease. It consists of regular sessions with a speech therapist. In order for a sick child to understand what movements need to be made to reproduce a word or sound, in certain cases, a speech therapist-defectologist manually stimulates the muscles of the vocal apparatus.
There are prospects for treating apraxia if it is carried out long and persistently. The child's speech will develop over time, but in rare cases the disease can be completely overcome. The period in which deterioration is observed will alternate with periods of improvement. This will happen all my life. During adolescence, when active growth occurs, deterioration can often be observed. This is due to the active growth of organs that are responsible for the functions of the voice (mouth, tongue, throat).
There are times when apraxia
takes very severe forms. Children need extra help to communicate with others. In these cases, it is necessary to use either sign language or high-tech devices whose functions include generating human speech. These devices have been a big breakthrough for people who suffer from severe apraxia.
Diagnosis and causes of apraxia
In general, there are several reasons that explain the appearance of all types of apraxia. The main cause is brain damage that occurs due to trauma or is a consequence of tumors and heart attacks. Localization of the lesion in the parietal lobes (degenerative process) also causes apraxia
. It is in this zone that all action patterns that are learned throughout the entire period of life are stored. Damage to brain regions such as the frontal lobe, corpus callosum, and premotor cortex becomes another cause of apraxia.
It is necessary to examine the patient and ask him to perform some basic steps to determine the cause of the disease. The doctor asks to clap your hands and wave your hand. During the examination, the specialist checks the muscle strength, which is observed in the muscle groups involved. This is required in order to understand whether paresis is the cause of the disorder. Neuropsychological examination is required when identifying a complex variant of apraxia. Consultation with an occupational therapist and a physical therapist can help establish an accurate diagnosis.
The attending physician talks to the patient’s relatives, asks them about how independent the patient is, whether he can perform basic actions himself. Can the patient use cutlery, a toothbrush, and scissors? Is he able to write and draw figures? To clarify the causes of the disease, magnetic resonance imaging and computed tomography are used, which makes it possible to establish an accurate diagnosis and understand the nature of the lesion. This could be hemorrhage, focal atrophy, heart attack, etc. Neuromuscular diseases are often identified and can be confused with apraxia .
Treatment
Many disease factors must be taken into account to understand the prognosis and which treatments should be used. The nature and extent of the lesion and the patient’s age are taken into account. In modern medical practice there is no specific treatment. Occupational therapy and physiotherapy are used, which can help the patient recover.
It should be taken into account that all drugs whose function is to slow the progression of dementia are not effective against apraxia. The patient's functions improve and his life becomes safe if physiotherapy is used.
Apraxia manifests itself in a violation of the ability to act purposefully. If motor skills are affected, the patient is unable to make himself a cup of coffee.
As a result of apraxia, children lose the ability to acquire household and other skills. Patience and perseverance are required in such a long and difficult process as treating apraxia.
It is necessary to immediately contact a neurologist or psychiatrist if there is the slightest suspicion of apraxia. The cause and type of disorder determine which specialist will carry out the treatment. In most cases, patients with apraxia
special, individually selected treatment measures are required. These include work with a speech therapist, vocational training, and physical therapy. Family members must remember that patients need constant care, help and support.
The patient needs a caregiver who can help organize outpatient treatment or ongoing care. A social worker is needed to help determine the resources needed for the patient and his family. And a psychologist is needed to provide consultations to family members to help them understand how to communicate and care for someone with apraxia.
Apitherapy and herbal medicine are effective. The following medicinal infusions can be used: hawthorn, coltsfoot, elderberry, caraway seeds, lingonberries, blue cornflower fruits, rose hips, chamomile, motherwort, wild strawberry, black rowan, yarrow, golden mustache, lemon balm.
Flower pollen and royal jelly are also quite effective. The chemical composition of flower pollen depends on which plant or flower it was collected from. Pollen contains albumins, enzymes, mucoproteins, stearins, amino acids, flavonoids, carotenoids, vitamins, 28 carbohydrates, macro- and microelements. Amino acids (histiine, lysine, methionine, leucine, tryptophan, valine) give pollen its unique properties. It is necessary to consume pollen 1-2 teaspoons once a day for one and a half months. Then a break is taken for two to three weeks, and the course of treatment is repeated again.
Varieties
Kinesthetic apraxia is divided into three main types:
- kinetic apraxia of the limbs or melokinetic apraxia;
- ideomotor;
- ideational.
Ideatorial kinesthetic apraxia is understood as a violation of extrakinetic engrams of memory, which contains a spatio-temporal ideational plan that determines the path that motor functions will follow, how the limbs and their parts will act, the sequence, rhythm and speed of movements.
This disorder provokes disturbances in unusual and complex actions, while the usual, simplest actions are preserved. Action formulas, which are stored in extrakinetic memory, guide such complex movements, using kinetic, tactile and primary visual abilities to carry out these movements. Damage to extrakinetic engrams or an obstacle that arises in the process of their formation contributes to ruptures and errors in the ideational concept, and sometimes to the absolute inability to realize them.
It is believed that articulatory kinesthetic apraxia is a consequence of a break in the connection between the extrakinetic store and the store of kinetic engrams, as well as a break in connection with new tactile, optical and acoustic stimuli, which contributes to the development of apraxia of single simple motor actions.
Causes of apraxia
Apraxia occurs when the functions of certain parts of the cerebral hemispheres are impaired. This dysfunction can occur if damage in the brain occurs across the neural pathways that store memories of learned movements. A person with apraxia is unable to access this information. Apraxia can occur due to a head injury or a disease that affects the brain, such as:
- dementia
- tumors
- corticobasal degeneration
Apraxia often occurs in older adults due to neurological conditions such as ischemic stroke and dementia. If apraxia occurs after a stroke, the condition may improve within a few weeks.
Apraxia can also be genetically determined.
Prevention
There are currently no effective preventive procedures aimed at preventing the development of kinesthetic articulatory apraxia. However, some effective recommendations can be identified that will significantly reduce the likelihood of developing the described disease:
- regular exercise and outdoor walks;
- cessation of drinking alcoholic beverages and smoking;
- normalization of diet;
- nutritional balance;
- regularity of medical examinations;
- blood pressure control.