Tuberculous meningitis is an inflammation of the meninges caused by Mycobacterium tuberculosis.
Our expert in this field:
Nagibina Margarita Vasilievna
Infectious disease doctor, MD
Call the doctor
Some numbers and facts:
- Around the world, about 2 billion people are infected with tuberculosis. This is approximately a third of the world's population.
- Approximately 10% of patients develop signs of tuberculous meningitis.
- The higher the incidence of tuberculosis in a society, the more cases of damage to the meninges of tuberculous origin.
- Despite all the advances of modern medicine, tuberculosis still remains one of the biggest global health problems.
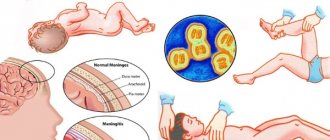
How does meningitis of tuberculous origin occur?
The disease develops in two stages:
- Initially, infection occurs by airborne droplets, the infection is localized in the lungs and nearby lymph nodes. Mycobacteria penetrate the blood and infect the pia mater.
- The pathogen then enters the cerebrospinal fluid and causes inflammation of the pia mater at the base of the brain.
About 80% of people who develop tuberculous meningitis have active tuberculosis or have had it previously. Other factors that increase the risk of the disease: HIV, alcohol abuse, decreased immunity caused by chronic diseases or taking drugs that suppress the immune system.
With tuberculous meningitis, the risks of severe complications and death are high. It is very important to establish a correct diagnosis in a timely manner and prescribe effective treatment. It is possible to understand what pathogen causes the disease only after a special examination at a neurological center.
Diagnostics
Hemogram (moderate leukocytosis and increased erythrocyte sedimentation rate, lymphopenia, eosinopenia, monocytosis).- Examination of the cerebrospinal fluid (the cerebrospinal fluid is opalescent, the protein content is increased, a fibrin film may form; lymphocytic pleocytosis, glucose and chloride levels are reduced; mycobacterium tuberculosis is detected in the cerebrospinal fluid).
- Sensitivity to tuberculin is reduced to the point of negative anergy.
- X-ray or computed tomography of the chest (detection of tuberculous lesions)
- Electroencephalography (epileptiform activity).
- Consultation with a neuro-ophthalmologist (tubercular rashes in the choroid, optic neuritis or fundus congestion).
Differential diagnosis:
- Other serous meningitis.
- Encephalopathies of other origins.
Treatment of tuberculous meningitis
Without appropriate treatment, meningitis leads to death. The patient should be immediately hospitalized in a specialized clinic and prescribed special anti-tuberculosis drugs. Often, glucocorticoids are prescribed along with them - drugs of the adrenal cortex that suppress inflammation.
Treatment lasts a long time, usually 12 months. After this, the patient should be monitored by a doctor, as there is a risk of relapse.
Meningitis caused by Mycobacterium tuberculosis cannot always be accurately diagnosed immediately, even by an experienced doctor. In this case, the disease is life-threatening. By self-diagnosis and self-medication, the patient loses time that could be spent on effective therapy. If you experience symptoms of the disease, immediately consult a neurologist. Call our clinic
The material was prepared by an infectious disease specialist at the Medicine 24/7 clinic, Doctor of Medical Sciences Margarita Vasilievna Nagibina.
Epidemiology of the disease
The most frequent outbreaks of infectious meningitis occur in winter and spring . The epidemic rise, as a rule, is recorded in November-December, the decline occurs in February-April.
Such activity in winter is explained by frequent temperature changes, high humidity (which is a favorable environment for the proliferation of viruses and bacteria) and the fact that in winter, people are forced to spend a long time together in closed, poorly ventilated rooms.
Risk group
Regarding infectious meningitis, the following groups can be distinguished that are most susceptible to infection:
- unvaccinated schoolchildren and children going to kindergarten during the winter period are exposed to large numbers of people for a long time, in poorly ventilated areas;
- people using public transport are in close proximity to possible carriers of infection for a long time;
- newborns whose mothers are carriers of meningococcal infection;
- people with weakened immune systems, especially HIV positive;
- people traveling or on business trips to places where outbreaks of meningitis have been recorded.
Infection statistics in the Russian Federation
Significant surges in the increase in incidence are observed in the Russian Federation every 10-12 years . The first serious outbreak of the disease on the territory of the USSR was recorded in the period from 1930 to 1940. During these 10 years, infectious meningitis was observed to affect 50 people out of 100,000.
The next epidemic occurred in the late 60s and early 70s of the 20th century. For every 100,000 people, there were 16-17 cases of meningitis. The cause of the epidemic was meningococcus, accidentally brought into our territory from China.
According to statistics, in 2014, per 100,000 children in the Russian Federation, there were 2.6 people infected with meningococcus. A total of 991 cases of acute meningitis were reported across the country.
In 2021, the number of diseases began to decline; compared to 2015, the total number of meningococcal infections fell by 20%. At the same time, the number of people sick with meningitis from enterovirus increased by 1.8.
Incubation period: how quickly does the infection develop?
It is impossible to answer with certainty how soon meningitis will develop.
It all depends on the type of bacteria and infection that became the root cause of its development. Eg :
- for meningococci, the incubation period averages 2-10 days, mainly after infection, the disease manifests itself on days 4-6;
- arenovirus, which provokes the development of lymphocytic choriomeningitis, can appear 5-12 days after infection;
- The development of meningitis caused by Haemophilus influenzae can occur at lightning speed, or it can proceed sluggishly over several weeks or even months.
The increase in morbidity and mortality from tuberculosis in the world and in Russia is due to the rapid spread of HIV infection [1-3, 10]. Since 2001, the highest rates of growth in the incidence of HIV infection in the world have been recorded in the Russian Federation. In total, in 2010, 509,734 people were registered in the country in whose blood antibodies to HIV were detected by immunoblotting. The total number of patients with tuberculosis in combination with HIV infection reached 24,963 people in 2010 - this is 5% of the number of patients with HIV infection. An important feature of the increase in incidence is the increase in the proportion of people with late stages of HIV infection: from 3.5% in 2005 to 11.4% in 2010, while 24,963 (5%) of them had active tuberculosis [7 , 10].
Until 2005, tuberculous meningitis (TM) was a fairly rare disease and was characterized by predominant damage to the membranes of the base of the brain [4, 6]. Due to the increase in the proportion of late stages of HIV infection from 2006 to the present, there has been a significant increase in the number of patients with TM, which necessitated the introduction of a new indicator into statistical reports [5, 9], reflecting the incidence of TM. Thus, in 2010 it was 0.13 per 100,000 population [5, 8].
The purpose of this work is to study the clinical features, diagnosis and pathomorphology of tuberculous meningoencephalitis (TME) in the late stages of HIV infection.
Material and methods
For the period 2007-2010. The results of observation of 140 patients were analyzed. The main group consisted of 120 patients with TME in the late stages of HIV infection (stage IVB). The comparison group included 20 patients with TM without HIV infection.
The average age of the patients was 30.5±8.5 years, 84.5% were men, 15.5% were women.
In 93.3% of patients in the main group, another localization of tuberculosis was simultaneously detected - damage to the lungs, all groups of lymph nodes, liver, spleen, kidneys, and less often other organs. 6.7% of patients had total damage to organs and systems. Respiratory tuberculosis was found in almost all patients.
TM without HIV infection proceeded mainly as an isolated lesion of the central nervous system; only 6 (30%) patients were diagnosed with disseminated pulmonary tuberculosis.
We studied X-ray data, the results of examining sputum and cerebrospinal fluid (CSF) for the presence of Mycobacterium tuberculosis using bacterioscopy, culture and PCR methods, immune status (CD4, CD8, CD4/CD8, viral load), determination of the content of protein, glucose, chlorides, cellular composition. CT and MRI of the brain were also performed.
In case of death, a pathomorphological examination was carried out in full in accordance with the established protocol. During autopsy, fragments of internal organs were fixed in 10% neutral formalin, processed according to standard methods, histological sections 3-5 microns thick were stained with hematoxylin and eosin, according to Van Gieson, Ziehl-Nielsen. Cytological preparations were studied with Romanovsky-Giemsa, Ziehl-Neelsen, and Gram stains. Immunohistochemistry (IHC) was performed using monoclonal antibodies to Myc. tuberculosis mouse
, clone 1.1/3/1, Vector.
Results and discussion
In 80 (66.7%) patients of the main group, the course of TME in the late stages of HIV infection was characterized by an acute onset without a clear prodromal period, hectic fever with the development of acute impairment of consciousness within 2-3 days from the onset of the disease, followed by the development of meningeal syndrome and symptoms of damage to the cranial nerves. In 40 (33.3%) patients, the onset of TME was asymptomatic or manifested by minimal symptoms and persistent changes in behavior - apathy, inadequate reaction to the environment, disorientation in place and time, partly in one’s own personality, impaired self-care skills, sometimes manifestations of aggression, a pronounced decrease in cognitive functions. In 20.2% of cases, a moderately severe cephalgic syndrome of a diffuse or local nature was observed.
TM without HIV infection was characterized by the presence of a clear prodromal period with the gradual development of intoxication syndrome, an increase in body temperature to febrile levels (90.2% of cases), increasing headache, up to unbearable (80.0%), often accompanied by nausea and no relief. relief by vomiting. Meningeal syndrome at the onset of the disease in patients of the main group was more often absent or mildly expressed, in contrast to TM without HIV infection (25.1 and 93.0%, respectively).
Damage to the cranial nerves in patients of the main group was observed 2.5 times less frequently than in the comparison group, which was obviously due to the convexital localization of damage to the meninges and substance of the brain. This is probably associated with more frequent cerebral and pyramidal symptoms and less pronounced meningeal syndrome.
Patients in the main group had severe immunosuppression: the number of CD4 lymphocytes was 100 cells/μl or less, the CD4/CD8 ratio was from 0.01 to 0.5, the viral load was from 500,000 cop/ml and above. The more acute the course of the disease, the lower the content of CD4 lymphocytes; CD4/CD8 ratio and higher - viral load. In fatal cases, the level of CD4 lymphocytes was 0-50 cells/μl, the CD4/CD8 ratio was 0.02-0.1.
In patients of the main group, the CSF, as a rule, revealed a moderate increase in protein (1-2 g/l), slight pleocytosis (on average 92±36 cells per μl) with a predominance of neutrophils (70-80%). In patients in the comparison group, the protein level in the CSF was significantly higher (from 3 to 10 g/l), pleocytosis reached 400-600 cells, mainly due to lymphocytes. Glucose levels in the main group decreased less significantly (1.3-1.9 mmol/l) than in the comparison group (0.7-0.9 mmol/l). The chloride content in the CSF did not differ significantly between the two groups. In patients of the main group, Mycobacterium tuberculosis was quite often detected in the CSF - by microscopy in 18 (15.0%) cases, culture - in 37 (30.8%), PCR - in 46 (38.3%), which is the most important criterion for diagnosing TM. It is extremely important to detect drug resistance of Mycobacterium tuberculosis in the CSF in 17 (45.9%) bacterial isolates, of which 9 (24.3%) had multiple drug resistance of Mycobacterium tuberculosis to drugs and 3 (8.1%) had extensive drug resistance. .
CT and MRI were used as an auxiliary diagnostic criterion for damage to the brain and membranes in 21 (17.5%) patients: foci of demyelination were identified in 13 (61.9%) patients, cerebrospinal fluid cysts - in 10 (47.6%), displacement of the median structures - in 5 (23.8%), decreased density of the brain substance - in 17 (81%), thickening of the meninges - in 2 (9.5%), impaired cerebrospinal fluid dynamics - in 18 (85.7%).
The study of the characteristics of the course of TME in patients of the main group made it possible to identify differences from the comparison group (see table)
.
Pathologically, TM without HIV infection was characterized by damage predominantly to the basal parts of the brain. The pia mater was jelly-like, swollen, with millet-like grayish miliary tubercles. TME revealed foci of caseous necrosis in the brain substance (Fig. 1)
.
Figure 1. Tuberculous meningoencephalitis in the absence of HIV infection. Caseous-necrotic focus in the substance of the brain, tubercular rashes of the pia mater. Unfixed macropreparation. Microscopically, in TM, in patients with a relatively intact immune status, the pia mater was edematous, with moderate fibrosis, vascular congestion, lymphoid infiltration of varying severity, miliary tubercles consisting of epithelioid cells, Pirogov-Langhans giant cells, with a lymphoid shaft along the periphery. Leukocytes could be detected in the inflammatory infiltrate. Tuberculous granulomas sometimes merged with foci of central caseous necrosis (Fig. 2)
. Figure 2. Tuberculous meningitis (without HIV infection). Fibrosis, pronounced lymphoid infiltration of the meninges, separately located and merging epithelioid giant cell granulomas with necrosis in the center. Hematoxylin and eosin staining. Uv. 200.
In case of TM in the late stages of HIV infection, a total lesion of the pia mater was determined, with the involvement of the convexital surfaces of the brain in the process of sheathing. Due to purulent impregnation, the membranes acquired a yellowish-greenish color (like a “purulent cap”), tuberculate rashes were not visualized (Fig. 3, 4)
.
Figure 3. Tuberculous meningitis due to HIV infection.
a - purulent impregnation of the membrane of the basal parts of the brain; b — damage to the membrane of the convexital surface of the brain. Unfixed macropreparations. Figure 4. Tuberculous meningitis due to HIV infection. a - in the pia mater there is pronounced edema, plethora, extensive purulent-necrotic foci without signs of granulomatous inflammation, pronounced vasculitis. Hematoxylin and eosin staining. Uv. 200; b — fragment with no signs of delineation of foci of tuberculous inflammation. Van Gieson staining. Uv. 200. With the development of TME, foci of destruction such as abscesses were identified in the brain substance. These changes give the impression of nonspecific bacterial inflammation, and only histological examination with additional stains and bacteriological examination can establish the tuberculous etiology of the process. In HIV-associated TME, the pia mater was edematous, sharply congested, with diffuse leukocyte, less often lymphoid-leukocyte infiltration. Purulent-necrotic lesions of a monomorphic structure with no signs of productive inflammation were located perivascularly (epithelioid and giant multinucleated cells were not detected in the vast majority of cases) (Fig. 5, 6)
.
Figure 5. HIV-associated tuberculous meningitis.
Abundance of acid-fast bacteria in the imprint smear of the pia mater. Ziehl-Neelsen staining. Uv. 1000. Figure 6. Mycobacteria in a purulent-necrotic focus of the pia mater. Immunohistochemical study with Myc. Tuberculosis mouse monoclonal antibody, clone 1.1/3/1, Vector. Uv. 1000. Purulent-necrotic foci similar to acute abscesses were also found in the brain matter. Characteristic was the development of vasculitis, including severe destructive forms, thrombovasculitis, which further intensified necrotic processes. In cytological preparations of impression smears of the pia mater and areas of brain destruction, as well as histobacterioscopically with Ziehl-Neelsen staining, a large number of acid-fast bacteria were found in necrotic masses and the cytoplasm of neutrophils (see Fig. 5)
.
Using additional histological stains, the tuberculous etiology of vasculitis was confirmed. Immunohistochemical reaction using Myc monoclonal antibodies. Tuberculosis mouse monoclonal antibody
made it possible to establish the generic affiliation of the pathogen and identify it as Mycobacterium tuberculosis
(see Fig. 6)
.
Thus, according to a pathoanatomical study of 56 people who died from TME with HIV infection, the following features of tuberculous brain damage in the late stages of this infection were established: generalized damage to brain tissue and meninges with multiple foci of necrosis and destruction of brain tissue in 51 (91.1%) sick; the absence of classic basal leptomeningitis and specific tuberculous inflammation, the formation of tubercles and granulomas, a specific shaft of epithelioid cells and Pirogov-Langhans cells in 48 (85.7%). Microscopy of material from foci of necrosis in 40 (71.4%) patients revealed a large number of Mycobacterium tuberculosis.
Here is one of our observations.
Sick, K
., 30 years old, was admitted to tuberculosis hospital No. 11 on December 12, 2008 with a diagnosis of HIV infection, stage IVB (AIDS). Generalized tuberculosis with damage to the brain and meninges (TME with right-sided pyramidal syndrome), lungs (disseminated pulmonary tuberculosis), damage to the intrathoracic lymph nodes.
Social status: unemployed with no fixed place of residence (lives in a rented apartment), low level of income. Height 175 cm. Weight 54.0 kg. Body mass index 17.6 kg/m2. Bad habits: smokes 1 pack of cigarettes a day, opium addiction.
History of the disease: tuberculosis was detected in June 2008, was treated in tuberculosis hospital No. 11 from June to November 2008, and was discharged with positive dynamics of the disease. After discharge he continued to use opiates. He did not receive antiretroviral therapy. The condition worsened in December 2008, when, against the background of general malaise, a high fever appeared and consciousness was impaired. On 12/07/08 he was urgently hospitalized at Infectious Diseases Clinical Hospital No. 2, where infiltrative tuberculosis of the lower lobe of the right lung and intrathoracic lymph nodes was detected. Then he was diagnosed with TME with right-sided pyramidal syndrome, infiltrative tuberculosis of the lower lobe of the right lung, intrathoracic lymph nodes, for which on December 12, 2008 he was transferred to tuberculosis hospital No. 11.
There were no complaints upon admission due to depression of consciousness (stupor). Rigidity of the neck muscles is moderately expressed. Severe Kernig and Brudzinski symptoms. Reacts by opening the eyes to loud speech and painful stimuli. Palpebral fissures D>S. The pupils are round in shape, D=S, reactions to light, and accommodation are reduced. The movements of the eyeballs are limited outward, there is no spontaneous nystagmus. The pharyngeal reflex is reduced. Right-sided hemiplegia with low tone. Tendon and periosteal reflexes of medium vivacity, S
X-ray of the lungs 12/15/08: on the right in the lower lobe there is a limited area of infiltration on both sides, increased pulmonary pattern, the roots are deformed, pleurodiaphragmatic adhesions on the right, the right dome of the diaphragm on the 5th rib.
MRI of the brain from 12/11/08 - multiple foci of hyperintense MR signal in T2 and TIRM modes, located on the right in the frontal and occipital lobes, on the left in the frontal lobe, most pronounced in the temporal (damage to the subcortical nuclei), parietal and occipital lobes. In the left temporal lobe there is a decrease in the MR signal in T1 mode from the pathologically altered substance. In the lesion on the left at the level of the precentral gyrus there is a focus of central necrosis. The left lateral ventricle is significantly compressed. Dislocation of the midline structures at the level of the third ventricle to the right by 7.8 mm, the fissures of the subarachnoid space are widened.
General blood test: hemoglobin Hb 108 g/l, erythrocytes 3.05·1012/l, leukocytes 6.9·109/l, platelets 37·109/l, monocytes 69, lymphocytes 27, ESR 65 mm/h. Biochemical blood test dated 12/08/08: total protein 80 g/l, total bilirubin 4.0 mmol/l, aspartate transaminase 23 U/l, alanine transaminase 16 U/l, urea 8.1 mmol/l, creatinine 64 µM/l, alkaline phosphatase 86 U, glucose 5.1 mmol/l.
General analysis of CSF: turbid, colorless, protein 2.32 g/l, glucose 1.2 mmol/l, chlorides 115 mmol/l, cytosis 32 (51% - neutrophils, 49% - lymphocytes) cells per μl.
Examination of the patient's biological materials for Mycobacterium tuberculosis: sputum and CSF bacterioscopy are negative. Culture of sputum and CSF for Mycobacterium tuberculosis - no growth. Mycobacterium tuberculosis was detected in the CSF using the PCR method.
Immune status: CD4 - 54 cells (12%), CD8 - 341 cells (57%), CD4/CD8 - 0.15.
Clinical diagnosis: HIV infection stage IVB (AIDS). Tuberculosis of multiple localization: tuberculous meningoencephalitis; infiltrative tuberculosis of the lower lobe of the right lung, MBT(-); tuberculosis of intrathoracic lymph nodes in the infiltration phase. Oral candidiasis.
Complications: edema and swelling of the brain. Cachexia. Respiratory failure of the 3rd degree. Pulmonary heart failure of the 3rd degree. Concomitant diseases: toxic-metabolic encephalopolyneuropathy. Liver cirrhosis of mixed etiology (viral and toxic).
The patient received anti-tuberculosis therapy - tavanic, rifadin, isoniazid, pyrazinamide, ethambutol, decongestant - mannitol, dexamethasone, detoxification - reogluman, hepatoprotective - karsil, as well as vascular, nootropic and antioxidant - Cavinton, piracetam, mexidol.
Despite the therapy, the patient's condition continued to deteriorate. Against the background of increasing symptoms of edema and swelling of the brain, death occurred on December 15, 2008.
Pathological diagnosis: HIV infection stage IVB. Generalized tuberculosis with damage to the intrathoracic and para-aortic lymph nodes, lungs (disseminated tuberculosis), brain (tuberculous meningoencephalitis with areas of suppuration), spleen (miliary), acid-fast mycobacterium tuberculosis are detected by all methods. Mycotic esophagitis. Brain edema with dislocation of stem structures. Pulmonary edema. Pulmonary heart failure of the 3rd degree. Addiction. Chronic viral hepatitis C. Cachexia.
A feature of this case was a significant predominance of encephalitis with the presence of gross focal symptoms and the development of dislocation syndrome. The disease occurred against the background of severe immunodeficiency.
In modern conditions, due to the increase in the later stages of HIV infection, there is a significant increase in the number of patients with TME, which, due to immunosuppression, has a severe clinical course with high mortality. In patients with TME with HIV infection, compared with patients with TME without it, a more acute onset of the disease, a predominance of symptoms of encephalitis confirmed by neuroimaging data, a more frequent detection of Mycobacterium tuberculosis in the CSF, and a high frequency of their multidrug resistance were noted. The microscopic picture of the TME in patients in the late stages of HIV infection does not have the specific features characteristic of tuberculous inflammation. Alterative-exudative reactions predominate in the absence of signs of granulomatous inflammation, which requires a morphological differential diagnosis between tuberculous brain damage and nonspecific bacterial inflammation.
Features of the clinical picture
Symptoms of tuberculous meningitis are divided into three stages:
- Prodromal period lasts up to 6-8 weeks. Symptoms appear gradually: apathy, lethargy, drowsiness, weakness, dizziness and frequent headaches, which gradually become stronger, the temperature rises to 38 degrees, nausea and vomiting begin.
- The period of irritation - the signs of the disease intensify, the temperature rises, headaches in the back of the head, constipation, photophobia, sound intolerance, the appearance and disappearance of spots on the body. On the 6-7th day of this period, meningeal symptoms occur: stiff neck, Kernig and Brudzinski's sign, hearing loss, vision problems, speech impairment, decreased sensitivity of the limbs, hydrocephalus, increased sweating and salivation.
- The terminal period is the last stage of the disease, paresis and paralysis begin, heart rate increases, loss of consciousness, difficulty breathing, temperature up to 40 degrees. The last stage of the disease ends in the death of a person.
In young children, symptoms are similar to those in adults, only their development occurs in an acute form and the periods are shortened.
The main symptoms characteristic of tuberculous meningitis developing in children are: on the 2nd day, convulsions, vomiting, fever may begin, the child screams, the fontanel swells and pulsates.
In older children, the onset of the disease is gradual, and the manifestation of symptoms is blurred. Meningitis can be determined by the way the child lies; if he constantly lies on his side, with his legs tucked to his stomach and his head tilted back - this is a sure sign of the disease.
Complications and prognosis
The consequences of tuberculous meningitis can be:
- neuroendocrine disorders (observed as a result of disruption of hormonal regulation of the glands);
- epileptic seizures;
- damage to the cranial nerves;
- relapses;
- motor and sensory disorders;
- encephalitis (inflammation of brain substances);
- dysarthria and dysphonia;
- optic disc congestion;
- visual disturbances;
- hearing loss;
- fecal and urinary incontinence;
- spinal cord damage;
- anorexia (extreme exhaustion);
- paralysis;
- paresis;
- heart rhythm disturbance;
- dehydration (occurs against the background of persistent vomiting);
- death.
Children at risk
More often, tuberculous meningitis develops in young children due to the lack of developed immunity or parental refusal to vaccinate against tuberculosis.
Mostly infants, weakened and premature children, as well as children from 3 to 5 years of age, are affected. Only in babies under one year of age the disease begins in an acute form, the temperature rises sharply, vomiting, convulsions begin, hydrocephalic syndrome and bulging of the large fontanel are noted.
In children older than one year, it usually begins with malaise, decreased appetite, and drowsiness. Then the temperature rises and vomiting begins - this happens within a week. Meningeal symptoms usually appear within 1-3 weeks.
For prevention purposes
The following preventive actions are distinguished to prevent infection with tuberculosis:
- vaccination before 30 days of life;
- early diagnosis of patients who have come into contact with the patient;
- isolation of a patient with tuberculosis in separate housing from an apartment building or dormitory;
- maintaining personal hygiene;
- regular examinations;
- undergoing fluorography;
- wet cleaning of the premises.
By taking precautions you can reduce the risk of infection. If it does happen, you should not self-medicate, but should urgently consult a doctor.