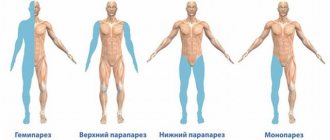
The concept of pseudobulbar dysarthria
In children, pathology is part of the complex of symptoms of cerebral palsy. Its formation is influenced by infections suffered during intrauterine development, birth injuries, and prolonged asphyxia.
Unlike true, bulbar dysarthria, with pseudobulbar dysarthria, changes do not affect the medulla oblongata. The nerve pathways responsible for the innervation of the articulatory apparatus are affected. Complete or partial paralysis of facial muscles occurs. The facial muscles are inactive, not only sound pronunciation suffers, but also the physiological acts of chewing and swallowing food.
With existing motor-speech problems, the mental abilities of such children are not initially impaired. The child perceives his own speech defects by ear and tries to correct them. Pseudobulbar dysarthria, in contrast to the bulbar form, is easier to correct and has a more optimistic prognosis.
Description of the disease
Pseudobulbar dysarthria is a speech disorder caused by paralysis affecting the articulatory muscles. They are constantly either in hypotonicity - relaxed, or in hypertonicity - overly tense. This occurs due to a rupture of the pyramidal tract, so the influence of the cerebral cortex on the spinal cord segments is disrupted.
Disruption of the connection between the speech apparatus and the central nervous system leads to a malfunction of the muscles responsible for the reproduction of sounds. Problems with the speech motor analyzer arise when there is bilateral damage to the corticonuclear pathways connecting the nuclei of the bulbar nerve endings.
In simple terms, this is a disease in which a child is physically unable to pronounce individual sounds and even words, or fully express his emotions. This usually manifests itself as follows:
- fast or too slow speech;
- unintelligible pronunciation;
- not saying the endings of words;
- distorted pronunciation of sounds or replacing them with others;
- unnatural inactivity of the muscles of the lower part of the face;
- open mouth
- involuntary flow of saliva.
Pathology develops with general lesions of the central nervous system of varying severity, for example, cerebral palsy. Changes manifest themselves in young children, mainly in disorders of sucking, chewing, swallowing, and respiratory dysfunction. It depends on the form of the disease.
A characteristic differential sign of the development of pseudobulbar dysarthria is precisely bilateral paralytic damage to the muscles of the tongue, palate, and larynx. As a result, there is a restriction of movement, articulation and phonation.
In some cases, with bilateral paresis, the degree of damage to one side of the organ may prevail over the other. Sometimes a whole series of involuntary movements are preserved, while voluntary ones simply disappear.
Causes of pseudobulbar dysarthria
Pathology always develops against the background of organic damage to nerve-conducting fibers. Bilateral spastic muscle paralysis develops. Thus, with an anatomically correct speech apparatus, conscious control of the muscles turns out to be impossible.
Like cerebral palsy, pseudobulbar dysarthria is associated with abnormalities of intrauterine development or a difficult birth process. The formation of pathology is influenced by:
- difficult pregnancy, aggravated by gestosis, fetal hypoxia, and Rh factor incompatibility;
- complicated labor;
- asphyxia during childbirth;
- intrauterine infections affecting the nervous system of the fetus.
In early childhood, dysarthria develops as a complication of previous conditions:
- infectious and inflammatory processes of the meninges;
- severe general intoxication;
- purulent-inflammatory pathologies of the ENT organs: sinusitis, otitis media;
- skull injuries.
Pathology can also overtake an adult with the following deviations:
- ischemic form of stroke;
- formation of atherosclerotic plaques, chronic brain hypoxia;
- damage to nerve fibers in multiple sclerosis;
- brain tumors of any etiology.
It is impossible to carry out full correction and restorative therapy without addressing the root cause. Therefore, treatment always proceeds in parallel.
Distortion of speech due to dysarthria
If a person is suspected of having bulbar dysarthria, he will need to undergo diagnostic testing to confirm the diagnosis. This can be done in a hospital setting; a medical specialist will listen to the patient’s complaints and decide what examinations to send for. Children will need to work with a speech therapist and neurologist. The first specialist will talk with the minor and assess the condition of the speech apparatus, as well as muscle mobility of the face. After this, the doctor will be able to make a conclusion about the condition of the child.
As you know, bulbar dysarthria is a disease that can affect the nervous system. That is why you will definitely need to contact a neurologist. The specialist will look at the conclusion made by the speech therapist and then examine the patient.
In addition, the doctor may prescribe various tests. Most often, the patient is referred for blood and urine tests, because deviations in the indicators indicate the presence of health problems. Electrography of the muscles of the neck, limbs and tongue is often performed.
Speech dysarthria is not considered an isolated disease. This is a symptom that manifests itself in a disorder of all speech characteristics: tempo, intonation, volume, consonance, clarity, etc. As a result, speech becomes slurred.
The cause of the disorder is damage to the parts of the central nervous system responsible for the innervation of the speech-motor apparatus. Dysarthria in adults can develop as a consequence of a stroke, tumor or brain injury. It also accompanies patients with amyotrophic and multiple sclerosis, Parkinson's disease, and occurs in mental retardation, neurosyphilis, and other pathologies affecting the brain.
A whole system of organs is involved in the formation of words. These are lips, tongue, cheeks, larynx, palate, respiratory and facial muscles. With dysarthria, these elements do not work in a coordinated manner. The reason for this is damage to the following nerves:
- sublingual;
- glossopharyngeal;
- facial;
- trigeminal.
In this case, inadequate functioning of the tongue is observed: limited movement of the tongue to the sides, up, down. He is in a tense state, which is why he gets tired quickly, and asymmetry of the lesion may be observed.
The cheek muscles also lack coordinated movements. This reduces the ability to correctly maintain posture when pronouncing sounds. Movement of the lower jaw is difficult. The lips are excessively compressed or, conversely, relaxed, the tongue lies at the bottom of the mouth, and the pliability of the soft palate is also impaired.
Motor stiffness, tension, paresis and paralysis of the facial muscles lead to the fact that speech
such a patient’s vision becomes incomprehensible, unclear and difficult to perceive. It is often characterized as porridge in the mouth.
Speech defects manifest themselves to varying degrees, depending on the area and extent of the lesion. There is an articulation disorder in pronunciation. A person does not pronounce almost all sounds, both vowels and consonants. Often hissing and whistling sounds have interdental or lateral pronunciation, the correct sound of voiced and hard consonants is lost, and defects in the pronunciation of “l” and “r” and sounds with posterior pronunciation appear.
Front-lingual letters (“d”, “t”, “z”, “s”) are pronounced with an interdental whistle. Complex sounds are replaced by simpler ones. Speech either unnaturally slows down, becomes drawn-out, or, conversely, accelerated. Gaps appear between letters and letter substitutions occur.
The voice also undergoes changes. It loses its volume, becoming quieter and weaker. The timbre becomes nasal and dull. Speech is monotonous, without emotional coloring. The intonation of the voice is lost: interrogative, narrative, exclamatory. Speech rhythm is inconsistent, stress placement is disrupted.
Due to problems with innervation, speech breathing also changes. During pronunciation it becomes more frequent, chaotic and intermittent. It’s as if the person doesn’t have enough air to finish the sentence.
Thus, speech impairment in dysarthria is polymorphic in nature, that is, it undergoes changes in all its characteristics. They are quite stable.
Diagnosis of the disorder is the prerogative of neurology and speech therapy. Instrumental research methods play a special role in making a diagnosis: EEG, electroneurography, electromyography, MRI, transcranial magnetic stimulation.
The speech therapist, in turn, must examine the condition of the speech-motor organs, facial and facial muscles. The specialist evaluates the nature of speech: how understandable it is for perception, the correct pronunciation of individual sounds, its tempo, rhythm, intonation, volume, synchronicity of the articulatory apparatus, and grammatical aspects.
Written speech is assessed by asking the patient to copy some text or take dictation.
Treatment of the disorder should begin with relief of the underlying disease. But speech disorders cannot be ignored.
It is advisable to begin correction of dysarthria as quickly as possible. Feeling his own conversational peculiarities, the patient will try to limit communication in society. This will lead to worsening of the speech defect. For example, from the first stage it will develop into the second. Isolation can also make it difficult to understand normal speech.
Therefore, in addition to treating the underlying disease, correction of speech defects is carried out. For this purpose, physiotherapy methods are used:
- various types of massage, including Shiatsu - influencing reflexogenic points using the finger method;
- acupuncture;
- physical therapy, including the use of special simulators;
- medicinal baths.
It is permissible for a psychoneurologist to prescribe psychotropic drugs as aids to normalize the psycho-emotional background.
Speech therapy treatment consists of using:
- speech therapy massage – working out the facial muscles. It allows you to improve blood circulation and restore normal muscle tone. Used to improve speech motor skills;
- exercises for voice production - the work of the vocal cords, volume and timbre of the voice are regulated;
- finger gymnastics – development of fine motor skills of the hands, which is interconnected with speech function;
- learning to position the organs of articulation for correct pronunciation;
- prosodic exercises - work on intonation, strength, height, tempo of the voice. Helps eliminate monotony;
- breathing exercises. Her exercises establish the correct breathing rhythm during speech activity.
Among the psychotherapeutic techniques used:
- art therapy;
- laughter therapy;
- clay and wax therapy;
- aromatherapy;
- music therapy;
- chromotherapy or color therapy.
Degrees of the disease
Depending on the depth of damage to the brain and neuromuscular system, 3 forms of pathology are distinguished. Each is accompanied by a certain severity of deviations and the possibility of correction:
- The lung is characterized by tense articulatory movements. The pronunciation of hissing and growling consonants is slow and requires effort, but in general the speech is understandable.
Facial movements are not fully preserved, but without obvious violations. The auditory perception of sounds is correct. There are no other motor impairments. The first stage can be easily corrected with systematic training.
- Average in prevalence takes the lead among children. There are difficulties in simple movements, maintaining the position of the tongue and lips. Speech is unintelligible with loss of syllables, words are pronounced “in the nose.” The facial expressions of the upper half of the face suffer, the movement of the eyebrows, and frowning is done with effort.
Constant, but insignificant salivation, the swallowing process is impaired. It is difficult for children to take care of themselves. Small movements, such as tying shoelaces and fastening buttons, are difficult to master.
This form requires long and painstaking work to restore functions. Children, as a rule, study in a correctional school. While mental abilities are preserved, the perception of sounds, and therefore spelling, is impaired.
- In the severe form, there is a complete speech disorder; it consists of individual sounds. There are no facial movements, the face takes on the features of a mask.
Muscle control is completely lost, the jaw drops, the tongue is immobilized. There is profuse salivation.
The disorders are predominantly bilateral, but sometimes asymmetry and a shift of paresis to the right or left half of the face are observed.
Manifestations of the disease
Deviations in speech motor skills
- Changes in the amplitude of movements - they become incomplete or completely impossible.
- The dynamic organization of speech has been changed - slow movements, a change in muscle tone from increased to decreased.
- Factor of impaired speech speed, which becomes slurred and blurred.
- Increased exhaustion of articulatory movements, which become inaccurate, incomplete, and each articulatory pose begins to be performed more than once.
- Symptoms include changes in muscle tone in the articulatory muscles, which inevitably leads to deterioration in sound pronunciation.
- Pseudobulbar dysarthria in children is primarily a deterioration in the pronunciation of front-lingual sounds, for example, “d”, “t”, “n” and so on, in combination with poor pronunciation of other groups of sounds.
Involuntary movements in children can be of three different types:
- hyperkinesis - violent automatic movements caused by spontaneous muscle contraction that occurs at rest and in motion;
- tremor – rhythmic short twitching of different parts of the body (limbs, head, tongue);
- synkinesis - additional motor activity added to voluntary ones.
Gross motor impairment
The muscular system of the whole body often acquires a tendency to hyperkinesis, accompanied by impaired coordination of movement. Such a child is less dexterous than his peers and begins to walk late. At the recovery stage, massage, rhythmics, exercise therapy, and logorhythmics help balance the condition. On the part of the facial muscles, there is problematic movement at the top of the face and smoothness at the bottom of the nasolabial folds.
As a secondary manifestation, there is a disturbance in sensations regarding the movements of the organs of articulation. Such children tend to have speech breathing disorders:
- Insufficient exhalation force.
- Small vital capacity of the lungs.
- Increased muscle tone in the chest area.
- Excessive saliva production.
- Marked acceleration of expiration.
Children with pseudobulbar dysarthria may experience disturbances in visual perception and spatial coordination. Work on speech therapy correction in such patients is always carried out comprehensively with the preparation of a detailed plan that takes into account drug treatment and the prescription of physiotherapeutic procedures.
Symptoms
Manifestations of pseudobulbar dysarthria can be noticed already in the newborn period:
- the child tensely sucks the breast or bottle, the movements themselves are given to him with effort;
- fatigue occurs during feeding;
- The baby is characterized by frequent choking and regurgitation.
Subsequently, a quiet, unintelligible babble is formed. Facial expressions are sluggish. There is a sharp change in the tone of the articulatory muscles: from excessive tension to complete relaxation. Speech development is delayed.
The first words appear after 2.5 years and are accompanied by a violation of the breathing rhythm. The child breaks up sentences with short breaths, which is due to increased tone of the chest muscles.
The baby speaks more often in one-syllable or two-syllable words. Most sounds are produced with tension, while the simplest reflexes: yawning, crying, smiling, licking lips are performed easily.
An imbalance between voluntary and reflex movements is a characteristic feature of pseudobulbar dysarthria.
Diagnostic measures
Diagnostic measures begin with an examination by a neurologist and speech therapist. Further management of children with disabilities is carried out by the same specialists. The patient is first referred to a neurologist. He conducts an examination, collects anamnestic data, and conducts additional examination.
Additional diagnostic methods:
- Electroencephalography.
- Electroneuromyography.
- Magnetic resonance imaging and other techniques.
After a complete neurological examination, the specialist makes a diagnosis and refers you for examination to a speech therapist. The speech therapist conducts a special examination, which includes an assessment of the functioning of the organs of articulation, facial expressions, and breathing during a conversation. He studies the patient’s anamnestic data, especially the stage of development of speech function (nature of sound reproduction, rate and clarity of speech). If the patient can write, the speech therapist evaluates the nature of the writing. Based on the results of the study, the specialist writes a speech therapy report.
Diagnosis of pseudobulbar dysarthria
Identification of pathology takes place in three stages. First, a pregnancy history is collected:
- the presence of early or late toxicosis;
- past infectious diseases;
- complications during childbirth;
- injuries.
Since pseudobulbar dysarthria is always accompanied by organic disorders, the functioning of the brain, nervous system, and muscle response is diagnosed. Basic methods:
- magnetic resonance examination;
- EEG;
- Electroneuromyography.
Psychological and speech therapy characteristics are of key importance. With pseudobulbar dysarthria, unlike other forms, it is meaningful actions that suffer. What does a speech therapist pay attention to:
- amplitude of tongue movement, performing precise exercises with the lips, holding positions for a sufficiently long time;
- oral speech: the range and complexity of spoken words, rhythm, intonation, correctness of sound, breathing when speaking;
- written speech.
An important role in diagnosis is played by differentiating pseudobulbar dysarthria from other types of pathology.
Diagnostic methods
To confirm pseudobulbar dysarthria, a number of studies are carried out, based on the results of which it is possible to draw a conclusion about a person’s well-being. First of all, a medical specialist will listen to the person’s complaints and conduct a visual examination. After this, the specialist will refer you to certain research methods that will help confirm or refute the diagnosis.
You will immediately need to go through the following procedures:
- Neurological examination. The doctor will test facial movements and articulatory motor skills. Determines the degree of limitation of facial expressions and the presence of pseudobulbar syndrome. The doctor will check for increased palatal and pharyngeal reflexes. It will be necessary to identify a neurological deficit, as well as establish the localization of the pathological process.
- Neuroimaging. Magnetic resonance imaging of the brain is most often used. With its help, it will be possible to understand whether there is a stroke, an inflammatory process in the cranial cavity, or degenerative changes. It will be possible to identify post-traumatic injuries and neoplasms. If there is an indication for MRI, a CT scan of the brain is performed.
- Cerebrospinal fluid examination. The collection is performed using a lumbar puncture. During the analysis, signs of neuroinfection can be identified.
- Speech therapy examination. A medical specialist will assess the condition of the articulatory organs and test oral and written speech.
- Assessment of cerebral hemodynamics. It is required if cerebrovascular insufficiency is suspected. According to indications, ultrasound, duplex scanning, and MRI of cerebral vessels are performed. If a problem with cerebral blood flow is identified, then such a condition will be considered background. It does not exclude the presence of other health problems.
- If necessary, you will need to visit a pediatrician, infectious disease specialist, geneticist and traumatologist. Based on the results of all studies, it will be possible to confirm or refute pseudobulbar dysarthria. If a person is diagnosed with this disease, then treatment will need to be started immediately to improve well-being. Only in this situation will it be possible to significantly improve the person’s condition.
There are different types of dysarthria: subcortical, erased, cerebellar, cortical, etc. To make an accurate diagnosis, consult a doctor.
Correction and treatment
Since the disease is complex, treatment is carried out in parallel in several directions:
- Medical treatments are aimed at combating the root cause. Nootropic drugs are used as medications. They improve blood supply to the brain, oxygen delivery, and activate biochemical processes.
Acupuncture and acupressure give noticeable results. The complex includes soothing baths and aromatherapy. To improve general motor skills - therapeutic exercises.
- Professional correction involves sessions with a speech therapist. With the help of articulatory gymnastics, the correct pronunciation of sounds, syllables, simple and complex words is worked out. The child learns to communicate expressively, use appropriate intonation, and his vocabulary expands. At the same time, fine motor skills are developing.
Both individual and group training have a positive effect. In the first case, the child is focused on completing the task correctly, and the allotted time is fully used for exercises. When studying in a group, the main factor is communication and socialization, conducting joint activities.
- Home training is aimed at consolidating acquired skills. They consist of a complex of articulatory exercises, which must be carried out several times a day, general gymnastics, and special massage of facial muscles.
Children with dysarthria benefit from communication with pets, creative arts, and water sports.
Treatment of the cause of the disorder and speech correction
The most important information is that pseudobulbar dysarthria can be corrected; after specialists (neurologist and speech therapist) determine the degree and form of the pathology, treatment is prescribed.
The neurologist prescribes:
- acupuncture (by influencing specific points, internal energy resources are activated);
- massage;
- physical therapy (its main goal is to strengthen the facial muscles);
- physiotherapy (magnet, paraffin applications, amplipulse, quartz, electrophoresis);
- drug treatment is aimed at activating the brain, improving the conductivity of nerve impulses, normalizing muscle tone, and the state of the nervous system.
A speech therapist helps develop:
- fine motor skills , which are extremely important for the development of speech, correct deficiencies by performing a series of exercises to develop accuracy, dexterity, and synchronization of movements;
- works with the speech apparatus : during the lesson, exercises are included that normalize the tone of the articulatory muscles, correct phonation is practiced, and the articulatory pattern of sounds is developed. Thanks to this, the degree of motor defects of the speech apparatus decreases;
- does breathing exercises;
- develops communication skills : a specialist helps to form grammatical skills, develop speech and help to master the use of words in speech.
In the treatment of pathology, treatment of concomitant diseases (cerebral palsy, tumors, meningitis, stroke, etc.), as well as support from family and friends, also plays an important role.
All family members should be aware of the problems of the disease and know the treatment methods and the program prescribed by the speech therapist and neurologist. This will help them support the patient and not control the proposed treatment option to achieve a quick and high-quality result.
Treatment of pseudobulbar dysarthria can be quite effective:
Forecast
Children with diction problems have always been and are a reason for ridicule among their peers. Therefore, in order not to complicate life for your child and yourself, you should determine the cause of speech disorders as early as possible. As the baby develops mentally and physically, his communication style develops. If adult family members understand him, do not make comments and do not seek help from a specialist, then the child is sure that he pronounces sounds correctly, although in fact this is not the case.
Pseudobulbar dysarthria detected at an early age makes it possible to correctly develop a treatment method and prevent progression of the disease. All children have a chance to recover, given the availability of modern interactive treatment methods.
Classes with a speech therapist are held in the form of an exciting game. The child himself does not notice when he begins to pronounce this or that letter or their combinations.
However, positive dynamics are not always observed. In severe forms of cerebral palsy, therapy does not give the desired effect.
In general, the prognosis for this disease is not very optimistic. It is almost impossible to completely restore the sensitivity of nerve endings. Patients with pseudobulbar dysarthria simply need to learn to live with their illness.
Varieties and their manifestations
In addition to the fact that there are several types of dysarthria, pseudobulbar dysarthria, in turn, occurs in the following forms:
1. Paretic . It is characterized by hypotonia of speech and general skeletal muscles. An increase in tone can be observed with voluntary movements. Paretic changes extend to the soft palate, labial and lingual muscles. Changing body posture is difficult and significantly slower. The movements of the articulatory apparatus are not synchronous with breathing. Excessive drooling or synkinesis is often present. If the voice is loud, then it quickly declines, becoming weak, monotonous, with a nasal tint. The pronunciation of sounds is blurred and unclear. Sucking and chewing reflexes are most often impaired, but not to critical levels.
2. Spastic . It is characterized by hyperkinesia of the muscles of the larynx and lips, spasmodic paresis of the tongue, and impaired tone of the soft palate. Speech is monotonous and nasal. Maintaining and changing articulatory posture causes difficulties; silent articulation is often present. The speech muscles are in constant tension; they are activated by spasms of the labial and tongue muscles. Sucking and swallowing cause certain problems, breathing is irregular and weak. The exhalation is short, and speech can be while inhaling. During spasmodic manifestations, the child cannot maintain the pace of conversation, so he deliberately uses short phrases or individual words. The meaning of speech is preserved, but intelligibility is quite low and depends on the voice data.
3. Mixed . The most common form of pseudobulbar dysarthria. The complexity of the disease lies in the fact that neighboring muscle groups are under varying degrees of tension. For example, the cheeks and lips are in increased tone, and the muscles of the tongue are not tense enough.
4. The most severe form is anarthria , which is characterized by deep muscle lesions and a complete absence of voluntary motor skills in both the speech and articulatory apparatus. The face of a child suffering from this form of the disease resembles a mask with its mouth constantly open. The tongue lies motionless at the bottom of the oral cavity, and lip movements are severely limited. Chewing and swallowing are difficult. There is no intelligible speech at all; sometimes the baby pronounces individual sounds. With pseudobulbar dysarthria, manifestations such as decreased muscle functionality of the tongue, hypersalivation, and choking are observed. These differential signs of the disease can be noticed already in the first year of a child’s life. Over time, other symptoms join them. In speech activity, the pronunciation of sonorant, whistling and hissing sounds suffers. These manifestations are characteristic of all forms of the disease.
Cerebellar dysarthria
Cerebellar dysarthria
caused by damage to the cerebellum, in which its connections with other parts of the central nervous system are disrupted. Speech in this form of dysarthria is slow, impulsive, chanting, with disturbances in stress, volume, and fading of the voice towards the end of the phrase (reminiscent of the speech of a drunk person). There is a decreased tone of the muscles of the tongue and lips. The tongue is thin, spread out, its mobility is limited, the pace is unhurried, the soft palate sags, chewing is weakened, and facial expressions are sluggish. The child cannot maintain an articulatory posture, and excessive or insufficient range of tongue movements appears. When straining and performing these movements, a tremor of the tongue is observed. The patient's medical history always includes PPCNSL.
Prosody and expressiveness of speech are disturbed, breathing is impaired. Most sounds are nasalized, the pronunciation of anterior lingual and labial sounds is impaired. A child with a cerebellar form of dysarthria usually speaks later than others. Features of general motor skills - movement disorder, the child often falls, many injuries. Most children have disproportionately large heads. Due to low muscle tone, the child has poor posture (possibly remnants of cerebral palsy), folds in half, and lies on the table. In most cerebellar dysarthrics, intelligence is preserved.
Up