What is the cerebral venous system
The vascular structure makes up 2/3 of the total volume of the cerebral bed.
The veins of the brain are a whole complex of sinuses, an anastomosis arranged in tiers inside the skull. It differs from the arterial one in that it has a much larger reservoir. Includes:
- capillaries;
- sinuses (large collectors);
- diploic, emissary;
- veins of the orbit, eyeball;
- jugular - a paired organ located on the neck, forming an upper hollow structure.
Basically, cerebrospinal fluid accumulates in the sinus sinuses with walls made of hard shell lined with endothelium.
A special feature of the structure is the presence of sinus canals that prevent compression of the cortex, although the tubes do not have a rigid frame. Therefore, the outflow of lymph can become difficult if the pressure of the cerebrospinal fluid begins to rise rapidly.
There are paired and unpaired sinuses.
The pair group includes:
- cavernous with location on both sides of the skull, starting from the Turkish ganglion
- sphenoparietal, extending downward from the main ossicle in the parietal lobe
- superior petrosal with origin at the cavernous sinus, extending along the edges of the pyramid of the temporal bone, flowing into the sigmoid region
- transverse, originating from the lateral confluence of sinuses
- sigmoid as a continuation of the transverse section with an S-shaped bend.
Unpaired:
- upper longitudinal, located at the site of attachment of the falciform process, collecting lymph from the bones of the calvarium and superficial components;
- lying below, collecting cerebrospinal fluid from the inner lobe of the convolutions of the gray matter and the corpus callosum;
- straight, passing along the line of junction of the tentorium of the cerebellum with the falciform process;
- occipital, originating from the occipital bone (internal tubercle), passing along the line of attachment of the falciform process.
Symptoms of the disease
Before rushing headlong into the pool, you should observe whether such prevention is required at all. The statistics of recent years are merciless - they clearly show how dangerous vasoconstriction really is. In addition, in recent years, this disease has become increasingly “younger” - if previously only older people suffered from it, today it also appears in young people. The reason is simple: the unfavorable environmental situation in large cities and bad habits.
Most often, the disease manifests itself quite clearly - its symptoms are very easy to notice. First of all, because the patient has to suffer from them literally every day.
Among the main signs of vasoconstriction are:
- increased fatigue;
- systematic headaches;
- decreased performance;
- noise in ears;
- memory problems;
- frequent fainting;
- dizziness.
You should not wait for all the symptoms mentioned to appear - even a few from this list should already be the reason for an early visit to the doctor
Remember: the consequences of the disease can manifest themselves in the form of a stroke or heart attack. For older people, there is another danger: against the background of the disease, they may actively develop senile dementia.
The consumption of strong drinks should be treated with the utmost care. They have the ability to dilate the veins for a short time, but subsequently the effect quickly disappears, the vessels narrow sharply and quite painfully.
As you can see, many of the problems mentioned also lead to increased cholesterol levels in the body. It will begin to deposit on the walls of the circulatory system, disrupting the elasticity of arteries and veins, interfering with patency.
Functions of veins
The system includes shallow and deep veins of the head.
The functions of the former include:
- outflow of cerebrospinal fluid, metabolic products and gray matter of the convolutions into the straight vein;
- outflow into the sinuses and then into the upper hollow, brachiocephalic region.
Through the deep veins of the brain, according to anatomy, blood is carried away to the external and internal jugular components, starting from the subcortical formations.
Well-developed baro-chemoreceptor structures are responsible for supplying information to the cerebral cerebellum regarding any changes in the composition of the cerebrospinal fluid and pressure.
Thanks to the many anastomoses located inside the medulla, unity of blood circulation and structural integrity are created in the area of superficial and deep capillaries.
Manifestation of the disease in a child
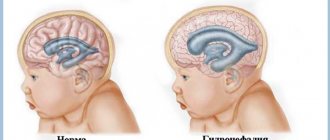
Abnormal development of the cerebral vascular system mainly occurs during the embryonic development of the fetus. If the pathology was not detected during pregnancy, it may not manifest itself for a long time. During the period of rapid development of the child’s body (puberty), specific manifestations of the disease are possible: causeless headaches, migraine attacks, convulsions. In severe cases, the child may have an epileptic seizure.
But sometimes the disease makes itself felt already in the first days of the baby’s life. A large area of deformed blood vessels in an infant can lead to congestive heart failure, which in turn leads to difficulty breathing. Congenital malformations are more likely to lead to hemorrhage than acquired anomalies.
At the slightest suspicion of the presence of pathological processes in the vessels of the brain, you should consult a specialist to diagnose the disease.
Anatomy of the superior veins
The superior veins are located on the surface of the cortex of the gray matter convolutions.
The composition includes varieties of smaller branches:
- medium – large, paired with passage in the central groove;
- the inferior veins of the cerebrum with their origin from the base, located in the region of the cerebellum below. This is a whole network of branches in the gyral cortex with the collection of cerebrospinal fluid, starting from the dorsolateral component;
- anterior, originating from the medial lobe of the gyri, extending to the base of the cephalic cortex, joining the large semi-tube with the sagittal canal from below;
- shallow, extending from the surface of the cerebellum;
- basal, located at the foot of the medulla, responsible for the functionality of the optic nerve.
Causes
In most cases, arteriovenous malformation of the brain is a consequence of impaired formation of the cerebral vascular network in the prenatal period. The genetic factor has not been proven, so heredity presumably does not play a role. Chronic diseases of the expectant mother, intrauterine infections, and increased background radiation have a negative impact on the development of the cerebral circulatory system in the fetus. A teratogenic effect is also caused by taking certain medications, intoxication, and the presence of bad habits in a pregnant woman (alcoholism, drug addiction, smoking).
The frequency of hemorrhages in children with cerebrovascular pathology of this type is low. The disease usually first appears after reaching 20 years of age. As the patient gets older, the risk of rupture of the formation increases. Acquired malformations are very rare, manifesting by the age of 50. Among the causes of the development of the disease are atherosclerotic, sclerotic changes in the vascular wall, as well as traumatic brain injuries.
Anatomy of the internal veins of the cerebral hemispheres
Internal veins form in the interventricular space, begin to bend around the shallow edge of the thalamus and bend back between the leaves of the ventricle.
The internal cavity is equipped with many inflows.
Basic:
- Thalamostriatal, passing between the thalamus, caudate nucleus in the intermediate sulcus for collecting cerebrospinal fluid, entering the area of the anteroposterior septum. As it moves back, it begins to join with the villous, into which the small capillaries of the vestibule flow.
- Lateral.
- Veins of the corpus callosum.
- Dorsal, posterior.
- The villous vein is one of the powerful ones, flowing into the large cerebral vein with the drainage of cerebrospinal fluid from the plexus of tubules of the lateral ventricles.
The deep areas of the brain stem include veins:
- midbrain;
- oblong;
- lateral, flowing into the large cavity and into the internal structures.
What it is
Normally, veins and arteries are connected by an extensive network of small capillaries. The function of the latter is to transfer nutrients from the blood to organ tissues. Diffusion is possible due to the single-layer structure of the capillary wall. With malformation, part of the capillary network is replaced by larger convoluted vessels. Most often, this tangle is a combination of veins and arteries - in this case we are talking about arteriovenous malformation of the cerebral vessels (abbreviated as AVM). Sometimes only one type of anomaly is observed.
Why is this pathology dangerous? If the size of the conglomerate is small, it may not manifest itself for a long time, but large formations are very dangerous. First of all, there is a risk of rupture, since the vascular wall of the malformation is deformed and thinned. The probability of such an outcome is up to 4% per year, with repeated hemorrhage occurring 2 times more often. Lethal outcome in case of rupture is 1 case out of ten, and permanent disability occurs in half of them. If, in addition to the malformation, there are aneurysms, mortality increases.
What are diploic veins and their characteristics
Diploic - wide tubes, but with thin walls and no valves. They lie in diploe channels. Located towards the base of the skull.
Diploic and meningeal veins are constantly in close contact with each other.
These veins include smaller branches:
- Frontal with location in the thickness of the frontal bone, flowing into the sagittal region. The functions include the supply of lymph to the supraorbital and superficial part of the sagittal canal.
- Anterior temporal, feeding the sphenoparietal sinus with cerebrospinal fluid.
- Occipital and temporal, flowing into emissary capillaries.
- Posterior temporal, flowing into the auricular vessel and the transverse sinusoid recess with a deviation back.
The functions include the collection of venous lymph from the temporal and parietal bones in the area of the mastoid emissary tube.
There are many areas of the brain - there are no less reasons to hit them!
The localization of the zone of brain damage, its nature and depth depend on the causes of the development of venous discirculation, and the symptoms expressing it also “dance” from them.
Frequent reasons for disorders of the venous outflow from the brain include:
- pulmonary, or cardiac, or pulmonary-heart failure;
- compression of strategically important extracranial veins, such as the internal jugular, innominate, superior vena cava;
- malignant or benign tumors of the skull and brain;
- TBI;
- thrombosis of the veins or sinuses of the brain;
- craniostenosis and dropsy of the brain, leading to compression of the veins;
- asphyxia of newborns;
- as well as a suicidal or violent reason - hanging.
Most often, this occurs due to thrombosis of veins of varying depths or venous sinuses of the brain (and the clinical manifestations of phlebothrombosis will not differ in any way from those with thrombophlebitis).
Description of the emissary
The emissary veins are located in the openings of the skull, connecting the capillaries of the cavity and the outer integument of the brain center.
Types of emissary branches:
- parietal, passing through the parietal foramen in the cerebellar region;
- occipital, surrounding the external occipital protuberance;
- condylar, located in the canaliculi of the occipital bone;
- mastoid, passing through the mastoid outlet of the temporal bone.
The emissary group includes not only tubes, but also plexuses - the foramen ovale, carotid and sublingual reflex.
Veins of the brain
The cerebral veins (vv. cerebri) are divided into superficial, forming in the cortex of the cerebral hemispheres, and deep, starting from the central parts of the cerebral hemispheres.
The following belong to the superficial veins of the brain (Fig. 416).
416. Veins of the brain. 1 - sinus signoideus; 2 - sinus transversus; 3 - confluence sinuum; 4 - sinus rectus; 5 - sinus sagittalis superior; 6 - vv. cerebri superiores
1. The superior veins of the cerebrum (vv. cerebri superiores) collect blood from the cortex of the dorsolateral surface of the cerebral hemispheres, forming a network of veins in the choroid. Large venous vessels are located mainly in the cortical grooves. Vv. cerebri superiores pierce the arachnoid membrane and flow into the sinus sagittalis superior.
2. The superficial middle vein of the cerebrum (v. cerebri media superficialisis) is a paired large vein that runs in the central sulcus and connects the sinus sagittalis superior and sinus cavernosus.
3. The anterior cerebral vein (v. cerebri anterior) originates on the medial surface of the cerebral hemisphere, extends to the base of the brain and connects the great cerebral vein with the inferior sagittal sinus.
4. The inferior veins of the cerebrum (vv. cerebri inferiores) originate in the basal cortex of the brain, flow into the sinus caroticus, intersigmoideus et. sphenoparietalis.
5. The basal vein (v. basalis) is formed in the area of the substantia perforata anterior, then accompanies the optic nerve tract. Having gone around the cerebral peduncles, it flows over the pineal gland into v. cerebri magna.
6. The superior veins of the cerebellum (vv. serebelli superiores) begin on the upper surface of the cerebellar hemispheres, flow into the sinus rectus and v. cerebri magna.
7. The inferior veins of the cerebellum (vv. serebelli inferiores) are located on the lower surface of the cerebellum and anastomose with the previous ones. They flow into sinus transversus and sinus petrosus inferior.
The internal veins of the cerebral hemispheres begin in the basal ganglia and white matter. They are represented by the following trunks.
1. The internal veins of the cerebrum (vv. cerebri internae) collect blood from the white matter of the cerebral hemispheres, the walls of the ventricles, the optic thalamus and the basal ganglia. In the transverse fissure of the brain near the quadrigeminal, all branches of the veins merge into the great vein of the brain (v. cerebri magna).
2. The vein of the choroid plexus (v. choroidea) is formed from the veins of the choroid plexus of the lateral ventricle, penetrating through the for. interventriculare into the central part of the lateral ventricle. It flows into v. cerebri magna.
3. The veins of the transparent septum (vv. septi pellucidi) begin in the substance of the brain, forming the anterior horn of the lateral ventricle. They flow into v. choroidea.
Great vein of the brain
The great vein of the brain (v. cerebri magna) is single, represents a short trunk 0.5-1 cm long. It is formed by the fusion of the above branches of the deep veins of the cerebral hemispheres. In the transverse sulcus of the brain above the superior colliculus, the midbrain flows into the sinus rectus.
Veins of the spongy substance of the bones of the cranial vault
Diploic veins (vv. diploicae) are located in the spongy substance of the bones of the cranial vault. They are oriented towards the large openings of the outer plate of the skull bones, through which the so-called exhaust veins (vv. emissariae) pass. The graduates anastomose with the saphenous veins of the skull, and the diploic veins with the venous sinuses. Due to the absence of valves in the veins of the spongy substance, blood flow through them is possible in two directions. The following diploic veins are distinguished.
1. The frontal diploic vein (v.diploica frontalis) is located in the scales of the frontal bone. Connects the supraorbital vein with the superior sagittal venous sinus.
2. The anterior temporal diploic vein (v.diploica temporalis anterior) is located in the parietal bone and the squama of the temporal bone. Connects the deep temporal veins and sinus sphenoparietalis, anastomoses with the frontal diploic vein.
3. The posterior temporal diploic vein (v.diploica temporalis posterior) connects the parietal outlet with the mastoid outlet and flows into the posterior auricular vein.
4. The occipital diploic vein (v. diploica occipitalis) begins in the squama of the occipital bone and flows into the occipital outlet.
Emissary veins of the skull
Emissary veins (vv. emissariae) are located in various parts of the skull.
1. The parietal emissary vein (v. emissaria parietalis) is a pair, connects the superficial temporal vein with the superior sagittal sinus.
2. The mastoid emissary vein (v. emissaria mastoidea) establishes an anastomosis between the sinus sigmoideus occipital and posterior temporal veins.
3. The condylar emissary vein (v. emissaria condylaris) connects the sinus sigmoideus with the venous plexuses of the spinal column and the deep vein of the neck.
4. The occipital emissary vein (v. emissaria occipitalis) is located on the external occipital eminence, reports vv. occipitales with the transverse sinus or the confluence of the sinuses.
Venous plexuses in the skull
The venous plexuses (plexus venosus) surround the contents of the foramen ovale, carotid and sublingual canals.
1. The venous plexus of the foramen ovale (plexus venosus foraminis ovalis) is located in the foramen ovale and connects the cavernous sinus with the pterygoid venous plexus.
2. The venous plexus of the carotid canal (plexus venosus canalis carotid) surrounds the internal carotid artery in the cranial canal of the same name, collects blood from the mucous membrane of the tympanic cavity and establishes a connection between the cavernous sinus and the pterygoid plexus.
3. The venous plexus of the hypoglossal canal (plexus venosus canalis hypoglossi) connects the occipital sinus with the sinus petrosus inferior and the internal vertebral plexus.
Veins of the orbit
From the contents of the orbit, the frontal region, and partly the upper jaw, small veins originate, which are the sources of the upper and lower ophthalmic veins, which flow into the cavernous sinus and veins of the head.
1. The nasofrontal vein (v. nasofrontalis) originates in the forehead and external nose. In the medial corner of the orbit it connects with v. angularis, representing the beginning of the facial vein.
2. Ethmoid veins (vv. ethmoidales) collect blood from the mucous membrane of the cells of the ethmoid bone, exit through the openings of the same name into the orbit.
3. The lacrimal vein (v. lacrimalis) originates in the lacrimal gland.
4. Veins of the eyelids (vv. palpebrales) and veins of the connective tissue membrane (vv. conjunctivales), vorticose veins (vv. vorticosae), ciliary veins (vv. ciliares), central retinal vein (v. centralis retinae), suprascleral veins (vv. episclerales) are formed in formations of the same name.
All of the listed orbital veins gather on the upper surface of the eyeball and merge into the superior ophthalmic vein (v. ophthalmic superior).
The superior ophthalmic vein has no valves and is characterized by a well-developed muscle layer. Initially, the vein is located in the medial corner between the superior and medial walls of the orbit, then it goes to the outer wall of the orbit, crossing the optic nerve under the superior rectus muscle of the eye. It leaves the orbit through the superior orbital fissure, flowing into the cavernous sinus.
The inferior ophthalmic vein (v. ophthalmica inferior) is formed from small veins of the lacrimal sac, medial, inferior rectus and oblique muscles of the eye. From the medial corner of the orbit, the vein passes to its lower wall and accompanies m. rectus inferior. In the upper part of the orbit, the vein divides into two branches: one of them flows into the sinus cavernosus or the superior ophthalmic vein, the other, passing through the inferior orbital fissure, connects with the deep facial vein. Anastomoses with the venous pterygoid plexus and the infraorbital vein. There are no valves in the system of these veins, so blood can pass both from the veins of the face to the cavernous sinus and back. This creates conditions for inflammation, when it is possible for infection to spread from the upper jaw, orbit and nasal cavity into the venous sinuses of the dura mater.
Veins of the meninges
Veins of the dura mater (vv. meningeae) originate in the dura mater and accompany the arteries. Veins from the shell of the calvarium flow into the sinus sagittalis superior, from the shell of the base of the skull into the venous sinuses of the base of the skull. Among the veins of the hard shell of the base of the skull, the middle vein (v. meningea media) is distinguished, accompanying a. meningea media. The vein flows into the sinus sphenoidalis and anastomoses in the area of the foramen ovale with the plexus of the same name and the pterygoid plexus.
Venous veins of the eyes and orbits
There are upper and lower venous veins of the orbit:
- The superficial ophthalmic one is the largest. It consists of the muscles of the shell of the eyeball, tissues of the nose and forehead, the vascular eyelid and capillaries that collect blood.
- Deep - located at the bottom of the orbit (under the optic nerve). It collects cerebrospinal fluid from the adjacent muscles of the eye and the vessels of the eyelid from below, then begins to move into the shallow eye cavity, which carries the blood to the cavernous canal.
Dyscirculation: when venous outflow is obstructed or impaired
The venous network of the brain is a reflexogenic zone with a high level of nervous organization, responsible for the course of the most important physiological processes that must ensure the constant blood supply to the brain.
“Dis-” means that the process is upset and out of control. When it comes to a circulation disorder, this indicates a more or less significant metabolic imbalance in the brain:
- oxygen;
- carbohydrate;
- water;
- fat.
And also about the increase in hypoxia and hypercapnia, venous and intracranial pressure, which leads to the development of cerebral edema.
The disorder of venous outflow goes through 3 stages along its path.
- In the latent stage, there are practically no complaints, no clinical symptoms are manifested.
- The period of cerebral venous dystonia is characterized by paraclinical changes; symptoms are few and do not interfere with life.
- A detailed picture of venous encephalopathy requires the intervention of a specialist, because it is already expressed by persistent organic microsymptoms.
According to the authoritative opinion of M. Ya. Berdichevsky, disturbance of venous outflow exists in two main forms:
- In the primary form , there is an increase in venous tone disorder; the basis for the development of venous discirculation is chronic nicotine or alcohol intoxication, hypertension or hypotension, venous hypertension or endocrine pathology, hyperinsolation or head injury.
- In the stagnant form, disruption of the flow of venous blood from the skull is caused by mechanical reasons, which leads first to a slowdown in venous circulation, then to stagnation of venous blood, and ultimately to cerebral edema.
Preventing problems
No less than in treatment for already developed pathology, the body also needs to prevent the problem of venous outflow - regular self-diagnosis.
An urgent examination by a neurologist and an ophthalmologist is necessary, with the necessary studies being carried out when:
- dull headache that gets worse with head movements;
- swelling of the lower eyelid;
- cyanosis of the cheeks, lips, nose;
- buzzing in the head with maximum manifestations in the morning;
- pronounced weather dependence;
- fainting, or dizziness, or blurred vision, not to mention mental disorders and epileptic seizures.
Measures to prevent disorders of the venous outflow from the brain also include maintaining an optimal work schedule, sleep and wakefulness, taking care of proper nutrition, and eradicating habitual intoxications and other harmful traditions from your life.
Other valuable methods of influencing the body in order to improve its condition are:
- various relaxation techniques;
- use of herbal medicine;
- taking a contrast shower;
- use of yoga.