Sensory aphasia is an acute disorder of neurogenic origin, in which there is a disorder in the perception of oral speech and a decrease in one’s own verbal abilities. Unlike other forms, the patient can still perceive some simple phrases addressed to him, but not always. It all depends on the severity of the deviation.
The patient hears everything, but does not understand what others are saying. To better understand what this looks like, it is enough to imagine that a person is surrounded by people communicating in a foreign language. Speech is perceived as something incoherent and incomprehensible, which is why anxiety and disorientation in space and one’s own personality develop.
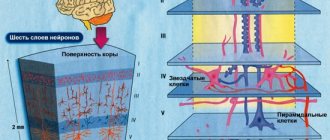
The classic cause of the development of such a pathological phenomenon was and remains a stroke. Speech perception in sensory aphasia is impaired due to damage to the temporal lobes. Especially if the so-called Wernicke center, responsible for oral speech and the perception of verbal information, suffers. Hearing is formally preserved, but it may decline or be completely absent in case of more extensive damage to the temporal lobes.
Diagnostics are carried out within the walls of the neurological department of the hospital under the supervision of a neurologist, and, if necessary, a neurosurgeon or vascular surgeon. Treatment depends on the root cause of the developed pathological condition. It is possible to carry out cerebrovascular therapy aimed at restoring normal trophism of brain tissue, surgery, and other forms of treatment. It is difficult to make predictions, but even in the case of a stroke, a quality result can be achieved in at least 60% of cases.
Classification of the disorder
Sensory aphasia occurs when the temporal lobes of the brain are damaged. But these structures are not homogeneous, they are complex, and therefore there may be several variants of the pathological process. For the ordinary patient, the classifications used by theorists and practitioners will say little. However, doctors actively use them when classifying sensory aphasia, developing treatment tactics, and predicting the prospects for a particular case. The main way to typify a disorder is to determine the location of the disorder and its mechanism. This is where the Wernicke-Lichtheim classification of aphasia comes to the rescue:
- Cortical sensory aphasia (also acoustic-gnostic aphasia). The classic and most severe type of disorder. Accompanied by damage to the so-called Wernicke's center, which is responsible for the perception of speech, sound stimuli, their logical processing and isolating what is essential from the surrounding sound noise. Accompanied by a total disorder of speech perception and reproduction.
- Transcortical form. It is accompanied by a disturbance in the conduction of nerve impulses between Wernicke's center and Broca's center, localized in the frontal lobe of the brain. At the same time, formally the ability to understand the simplest structures can be preserved, at least partially. However, the semantic connections of words in a sentence are incomprehensible to the patient; he cannot reproduce them himself. It is possible to develop pseudohallucinations, the notorious “voices” in the head, which have a complex compensatory origin (thus, the brain tries to get out of the information vacuum by creating false stimuli on its own).
- Subcortical sensory aphasia. Happens frequently. It is accompanied by a disturbance in the conduction of impulses from the centers that actually perceive sound information and the Wernicke center, which acts as a kind of processor, a processor of information and its transformation into understandable logical concepts and judgments.
There is also a conductive form, which is accompanied by disruption of connections between motor and sensory centers; it is difficult to distinguish it from cortical sensory aphasia, because they have a lot in common within the clinical picture.
Typing based on the severity of sensory aphasia is possible. There is no strict division within the framework of this criterion. The doctor assesses the degree of disorder by trying to communicate with the person. A patient with sensory aphasia either does not perceive speech at all, or reacts only to the simplest monosyllabic instructions and commands, which indicates a relatively lower severity of the disorder.
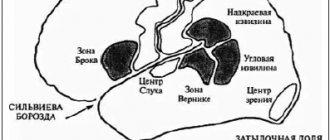
Scheme of localization of different forms of aphasia in the left hemisphere of the cerebral cortex
It is mandatory to evaluate hearing and the ability, in principle, to perceive sound stimuli. It is not necessary to refer the patient to an audiologist; this issue is resolved at the discretion of the neurologist. Based on the results, a simple form of sensory aphasia is distinguished (when only higher nervous activity is impaired) and a combined form (both hearing and the processing of verbal information are affected). Moreover, in the second case, it is hearing impairment that plays a possibly greater role, because the patient is not able to adequately perceive sound stimuli.
Reasons for the development of sensory aphasia
Development factors are very different. In most cases, we are talking about structural disorders of the brain, organic lesions. Few other options are possible. Some of the reasons include:
Stroke
Acute cerebrovascular accident. Accompanied by the death of nerve tissue and entire areas of the cortex. Depending on the extent of the lesion, we can talk about one or another severity of the disorder. Large-scale destruction is accompanied by total disturbances of higher nervous activity. As a rule, everything is not limited to aphasia. The development of sensory aphasia after a stroke is almost an obligatory sign of damage to the temporal lobes. Other symptoms, such as short-term epileptic seizures, are also detected. There may be some degree of hearing loss. Rehabilitation allows for successful restoration of verbal functions in 55-80% of cases or more.
Meningitis, encephalitis
Neuroinfections of varying severity. They provoke inflammatory processes in the brain and gradual tissue death. With a long course of the pathological process without proper treatment, massive structural changes in the brain are observed that cannot be corrected or reversed. Urgent treatment is required.
Hepatic encephalopathy
A disorder of the brain due to liver dysfunction, usually acute hepatonecrosis or increasing symptoms of cirrhosis. In the second case, it is possible to influence the patient’s condition if appropriate treatment of the underlying disease is started and the destruction of nerve tissue is corrected.
Cerebrovascular insufficiency without signs of stroke
Chronic disorder of brain trophism. Accompanied by a gradual increase in the phenomena of sensory aphasia, and not always. Preventing the disorder is not difficult if you start timely treatment.
Cerebrovascular insufficiency, transient ischemic attack
She's a micro-stroke. Accompanied by pronounced signs of a classic stroke. When the temporal lobes are damaged, speech impairment, perception of verbal information develops, and complete or partial hearing loss is possible. The main difference from a classic stroke is the ability of spontaneous regression of a transient ischemic attack. That is, it goes away on its own even without medical help. In addition, it does not leave a permanent neurological defect. Everything is back to normal. But a micro-stroke is an alarming sign. He indicates that complete necrosis of brain tissue will soon occur.
Brain injuries
Various. From banal bruises and concussions to the formation of a hematoma that compresses cerebral structures. After emergency care and treatment, complete restoration of normal neurological functions is possible without loss of quality.
Vascular formations
Malformations (pathological areas of communication between arteries and veins), aneurysms. They are of congenital or acquired origin. Require surgical treatment. They may not show themselves for a long time. Sensory aphasia is an atypical variant of the course of the deviation, but quite possible. After surgical correction there is every chance of full recovery.
Tumors of cerebral structures
Usually we are talking about meningiomas that compress nerve tissue at the level of the temporal lobes. The second most common gliomas, they can be benign, but are more often malignant. On the third - tumors of the third ventricle. Including common pituitary adenomas, growing in an atypical manner, which also compress the temporal lobes. After removal of the neoplasia, as a rule, everything returns to normal after a few days or weeks. A course of rehabilitation may be required.
Among the inorganic causes can be called true epilepsy, not associated with neoplasms and other causes. When the factor in the development of the disorder is excessive electrical activity of the brain. In this case, memory impairment, tonic-clonic seizures with severe severe convulsions and loss of consciousness develop. Sensory aphasia is present before the attack, during the episode itself, and for some time after it (up to an hour or two), until the nervous functions are fully restored. Treatment is aimed at correcting the condition and preventing further attacks. There is no point in specifically and purposefully influencing sensory aphasia.
Nutritional Features
The course of treatment for aphasia is long and difficult, therefore, when starting treatment, the patient and his entire family must be well prepared for a difficult battle for health. To achieve a 100% result from treatment, you need constant sessions with a speech therapist, psychologist, neurologist, and a wholesome, healthy diet. During treatment, the patient's brain is constantly working.
The patient may often sit in one position studying letters or reading a book. The diet of a patient with aphasia must be special. A person with this disease should have five meals a day, that is, he should eat food in small quantities and often.
You need to include in your diet something that helps your brain work well:
- Shrimp, lean fish; all seafood saturates the body with fatty acids, which help good attention and memory;
- Onions - it overcomes fatigue and nervous tension well, thins the blood, which further supplies the brain with oxygen;
- Nuts perfectly calm the nervous system due to their high content of vitamin B; fresh fruits, berries, especially avocados, bananas, blueberries, cranberries, strawberries, cabbage, beets, spinach, lemon, pineapple and others;
- Lean meat (beef, chicken);
- Dairy products (cottage cheese, yogurt, kefir);
- Legumes, cereals and pasta.
The breakfast of a patient with this disease should consist of 20% of the daily diet, for example, muesli with yogurt, porridge, boiled egg, second-grade bread, fruit. For an afternoon snack, you can have a small snack of some fruit or eat 100 - 200 grams of any nuts and drink drinking yogurt, kefir, tea with lemon. Lunch should consist of 40% of the daily diet, for example, a fresh vegetable salad, a piece of lean meat with potatoes, porridge, fresh berry compote or juice. For dinner, a piece of lean meat or fish, a vegetable salad, some fruit, or kefir is suitable.
The diet helps the brain function well, which helps quick reactions, thinking, and therefore a speedy recovery from such an unpleasant disease and the acquisition of full speech.
Symptoms
Symptoms of sensory aphasia include typical neurological signs and psycho-emotional disorders, which are secondary and caused by the difficult situation in which the patient finds himself.
- Inability to perceive speech. With intact hearing (in most cases), a person cannot make out what others are saying. Speech is heard, but it is not understood. It was as if the patient was surrounded by foreigners. This is the most complex version of the disorder. In lighter forms, the ability to perceive some simple structures is retained. Monosyllabic or phrases.
- Inability to speak independently. There are different levels of speech impairment. In classic cases, a person is able to speak, but in short phrases or even individual simple words. At the same time, he poorly understands what he himself is saying. In the most advanced forms, total speech dysfunction is observed. The patient makes inarticulate sounds. Features of the speech of patients with sensory aphasia are fragmentation, lack of clear logical connections, and the most poor lexical and grammatical structure. Usually these are fragmentary words and phrases.
- Psychomotor agitation. Accompanied by increased physical activity. The patient rushes about, cannot find a place for himself. A panic attack is possible. Severe attack of fear, panic.
- Aggressiveness, hostility. Within the framework of preserved consciousness. The affect of anger is associated with anxiety and lack of understanding of what is happening. Assistance is required; if necessary, an injection of a sedative is prescribed.
Additional symptoms are usually not associated with sensory aphasia and have a concomitant neurological origin. These are epileptic seizures with impaired consciousness, convulsions, loss of visual acuity, disruption of normal visibility, loss of individual fields of vision (scotoma). Verbal hallucinations are also common. Pseudohallucinations, when a person hears voices in his head. Paradoxically, the patient is not able to interpret even imaginary hallucinatory images; they are felt as auditory stimuli of a speech nature with incomprehensible content.
Signs of sensory aphasia persist throughout most of the period of the pathological process.
Game methods of correction in children
During correctional work, in addition to drug therapy, a speech therapist must work with the child; basically, classes are conducted individually. A specially selected technique activates individual affected areas of the central nervous system. The teaching material that is most often used:
- various texts;
- cards;
- Pictures;
- computer programs;
- items.
The speech therapist also uses options for everyday situations in which the child has an important role, and offers to listen to a musical composition or song. Exercises are given for listening and repeating counting rhymes, proverbs, nursery rhymes, and famous short poems. Classes must be conducted in a friendly and emotional manner, involving the child in the game process.
Parents are also recommended to do various speech therapy exercises with their child at home; the effectiveness of work to correct the disease depends on this.
Diagnostics
Diagnosis is carried out in a hospital setting. At the initial stage, an initial examination by a neurologist is indicated. Since the patient cannot answer questions, the presence of a relative or someone who can answer some questions for the patient is desirable, but this is not necessary. Typical primary signs are also noticeable: anxiety, excitability, misunderstanding of speech, difficulties with speaking.
A routine neurological examination is mandatory. The simplest basic reflexes are tested.
As part of the assessment of the general condition, the severity of damage to cerebral structures, and the nature of such, a group of instrumental measures is prescribed.
MRI is the basis and gold standard for diagnosis. Aimed at visualizing neural tissue. Allows you to diagnose all structural disorders. If necessary, targeted tomography of individual areas of the brain is prescribed. Especially the temporal lobes. Gadolinium contrast enhancement is often used. The drug accumulates in the changed tissues and enhances the pattern. Contrast is indispensable when diagnosing tumors. Infrequently, sensory aphasia is also possible with multiple sclerosis, which will also be clearly visible on post-contrast images in all details. For high-quality diagnostics, you need a high-field device with a power of 1.5 Tesla. If possible. Low-field ones will provide less data.
MRI of the brain
If vascular neoplasms are detected, angiography is additionally performed to better visualize the disorder.
Dopplerography of the neck vessels and duplex scanning of the brain are mandatory to assess the degree of blood flow in the cerebral structures. This will allow you to detect cerebrovascular insufficiency and assess its severity.
Specialists whose help will also be required are a neurosurgeon, a vascular surgeon. The characteristics of sensory aphasia within a specific medical history should be as detailed as possible in order to determine the type of pathological process and its features. Without this, there can be no effective treatment.
What can be concluded?
Although sensory aphasia is a problem that can happen to anyone, there is no need to lose hope.
You can take preventive measures: monitor your blood pressure, avoid head injuries, and consult a doctor if you suspect or feel worse.
With a disorder, a person does not forget how to speak completely , but it is difficult to perceive the oral speech of another person, and his own vocabulary is poor, and his thoughts are confused.
However, with the help of a speech therapist and psychologist, speech can be gradually restored, the main thing is persistence and a positive attitude.
Treatment
Therapy is also carried out in a hospital. In the early stages, treatment includes several stages: primary care immediately after admission to the hospital (especially if the patient is in serious condition), early measures aimed at relieving symptoms and combating the root cause, late stage and, finally, rehabilitation.
Nootropic drugs (Glycine, others), as well as cerebrovascular, antihypoxic medications (Piracetam, Actovegin and their analogues) are used. Often this is enough if the case is not advanced. Long-term use of medications is possible. For malformations, aneurysms, and tumors, surgical treatment cannot be avoided. It is necessary to remove them and restore normal tissue trophism, eliminating compression (squeezing).
Injuries with the formation of hematomas require drainage, that is, removal of the blood clot itself.
Epilepsy is a separate problem. The only way to correct the disorder is to systematically use antiepileptic medications as prescribed by a doctor.
Even after quality treatment in severe cases, usually post-stroke, neurological deficits remain. The patient still speaks poorly and does not perceive speech well. The issue is being resolved as part of rehabilitation. It takes from 6 to 12 months, rarely a little more. The time it takes to achieve results is 2 years. This is just a period of adaptation, restructuring the brain in a new way. Then achieving any effect is difficult or even impossible.
Exercises for semantic aphasia (sensory) are quite simple:
- reading and pronouncing simple words;
- delimitation of similar-sounding terms;
- the relationship between the image and the name of the depicted object;
- dialogues, at first simple, then increasingly complex.
Recovery is a routine and unpleasant task for the patient. But necessary. Depending on the quality of assistance, we can talk about one or another intensity of recovery.
Correction of deviations in Wernicke's aphasia is carried out according to indications. Usually everything is limited to the systematic use of cerebrovascular drugs, nootropics, and angioprotectors.
Exercises
The following exercises are recommended for therapeutic purposes:
- Working with subject pictures: classification of images by their names, characteristics, general categories.
- Selecting the correct name from several suggested ones.
- Differentiation of words that sound similar.
- Correlating images and text: writing stories based on pictures.
- Answers to questions: first they receive monosyllabic answers, then they practice dialogues from simple to more detailed ones.
- Reading and Writing: Start with individual letters and syllables, which are then put into words. Then they write simple dictations. Reading aloud begins with small texts, gradually moving to more extensive works. They master retelling and answer questions about the content of the text.
Prognosis and prevention
In 60% of cases with a stroke, it is possible to achieve lasting improvement or complete recovery (some authors talk about 80%). For other structural changes, we are talking about an 85% probability of complete recovery. If epilepsy is corrected, speech normalization is achieved in 98% of situations without any consequences
There is no prevention as such. It is enough to visit a neurologist from time to time for a preventive examination.
You may also be interested in: