Cortex
Cortex
is the outer layer of the brain, or gray matter.
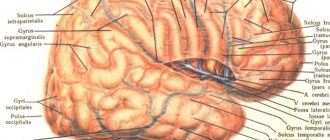
In humans, the gray matter has an uneven surface with many folds. Ridges called gyri
and folds called
sulci
help increase the surface area of the cerebral cortex.
The cerebral cortex contains four main lobes:
- frontal lobe
- parietal lobe
- occipital lobe
- temporal lobe
Since the hemispheres do not have clearly defined divisions, neuroscientists divide the lobes conditionally on the basis of grooves.
Central sulcus
(lat. sulcus centralis cerebri) is also known as the Rolandic fissure - a large groove in the cerebral cortex that separates the frontal lobe from the parietal lobe.
Precentral gyrus
— is located in front of the central sulcus, which neuroscientists use to identify the primary motor cortex of the brain.
Postcentral gyrus
— is located just behind the central sulcus, which neuroscientists use to identify the primary somatosensory cortex of the brain.
Lateral sulcus
- separates the temporal lobe from the frontal and parietal lobes.
Superior temporal gyrus
- located below the lateral sulcus, where the brain receives and processes information.
Fifth beat
, called
the insula,
is located inside the lateral sulcus.
Hemispheres
The longitudinal fissure divides the cerebral hemispheres into the right and left hemispheres. Each hemisphere controls processes on the opposite side of the body. This means that the right side of the brain receives and controls signals from the left side of the body, and the left side of the brain receives and controls signals from the right side of the body.
Although both hemispheres control many functions, some functions occur predominantly in one or the other. For example, the left hemisphere controls functions such as speech, writing, and mathematics. The right hemisphere controls aspects of creativity such as art and musical skills.
Structure
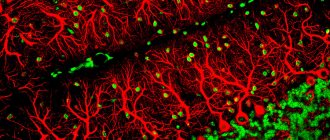
The cerebral cortex is a multilayered formation: each layer has its own specific composition of neurocytes, a specific orientation, and location of processes.
The systematic position of neurons in the cortex is called “cytoarchitecture”; fibers located in a certain order are called “myeloarchitecture”.
The cerebral cortex consists of six cytoarchitectonic layers.
- Surface molecular, in which there are not very many nerve cells. Their processes are located within itself, and they do not go beyond.
- The outer granular is formed from pyramidal and stellate neurocytes. The processes emerge from this layer and go to subsequent ones.
- Pyramidal consists of pyramidal cells. Their axons go down, where they end or form association fibers, and their dendrites go up into the second layer.
- The internal granular cell is formed by stellate cells and small pyramidal cells. Dendrites go to the first layer, lateral processes branch within their layer. Axons extend into the upper layers or into the white matter.
- The ganglion is formed by large pyramidal cells. The largest neurocytes of the cortex are located here. Dendrites are directed into the first layer or distributed in its own. Axons emerge from the cortex and begin to become fibers that connect various sections and structures of the central nervous system with each other.
- Multiform - consists of different cells. Dendrites go to the molecular layer (some only to the fourth or fifth layers). Axons are directed to overlying layers or exit the cortex as association fibers.
The cerebral cortex is divided into regions - the so-called horizontal organization . There are 11 of them in total, and they include 52 fields, each of which has its own serial number.
Vertical organization
There is also a vertical division - into columns of neurons. In this case, small columns are combined into macrocolumns, which are called a functional module. At the heart of such systems are stellate cells - their axons, as well as their horizontal connections with the lateral axons of pyramidal neurocytes. All nerve cells of the vertical columns respond to the afferent impulse in the same way and together send an efferent signal. Excitation in the horizontal direction is due to the activity of transverse fibers that follow from one column to another.
He first discovered units that unite neurons of different layers vertically in 1943. Lorente de No - using histology. This was subsequently confirmed using electrophysiological methods in animals by V. Mountcastle.
The development of the cortex in intrauterine development begins early: already at 8 weeks the embryo has a cortical plate. First, the lower layers are differentiated, and at 6 months the unborn child has all the fields that are present in an adult. The cytoarchitectonic features of the cortex are fully formed by the age of 7, but the bodies of neurocytes increase even up to 18. For the formation of the cortex, the coordinated movement and division of precursor cells from which neurons appear is necessary. It has been established that this process is influenced by a special gene.
Horizontal organization
It is customary to divide the areas of the cerebral cortex into:
- associative;
- sensory (sensitive);
- motor.
Scientists, when studying localized areas and their functional characteristics, used a variety of methods: chemical or physical irritation, partial removal of brain areas, development of conditioned reflexes, registration of brain biocurrents.
Sensitive
These areas occupy approximately 20% of the cortex. Damage to such areas leads to impaired sensitivity (decreased vision, hearing, smell, etc.). The area of the zone directly depends on the number of nerve cells that perceive impulses from certain receptors: the more there are, the higher the sensitivity. Zones are distinguished:
- somatosensory (responsible for cutaneous, proprioceptive, vegetative sensitivity) - it is located in the parietal lobe (postcentral gyrus);
- visual, bilateral damage that leads to complete blindness, is located in the occipital lobe;
- auditory (located in the temporal lobe);
- gustatory, located in the parietal lobe (localization - postcentral gyrus);
- olfactory, bilateral impairment of which leads to loss of smell (located in the hippocampal gyrus).
Disruption of the auditory zone does not lead to deafness, but other symptoms appear. For example, the inability to distinguish short sounds, the meaning of everyday noises (footsteps, pouring water, etc.) while maintaining the differences in sounds in pitch, duration, and timbre. Amusia may also occur, which is the inability to recognize, reproduce melodies, and also distinguish between them. Music can also be accompanied by unpleasant sensations.
Impulses traveling along afferent fibers on the left side of the body are perceived by the right hemisphere, and on the right side - by the left (damage to the left hemisphere will cause a violation of sensitivity on the right side and vice versa). This is due to the fact that each postcentral gyrus is connected to the opposite part of the body.
Motor
Motor areas, the irritation of which causes muscle movement, are located in the anterior central gyrus of the frontal lobe. Motor areas communicate with sensory areas.
The motor tracts in the medulla oblongata (and partly in the spinal cord) form a decussation with a transition to the opposite side . This leads to the fact that irritation that occurs in the left hemisphere enters the right half of the body, and vice versa. Therefore, damage to the cortex of one of the hemispheres leads to disruption of the motor function of muscles on the opposite side of the body.
The motor and sensory areas, which are located in the area of the central sulcus, are combined into one formation - the sensorimotor zone.
Neurology and neuropsychology have accumulated a lot of information about how damage to these areas leads not only to elementary movement disorders (paralysis, paresis, tremors), but also to disorders of voluntary movements and actions with objects - apraxia. When they appear, movements during writing may be disrupted, spatial representations may be disrupted, and uncontrolled patterned movements may appear.
Associative
These zones are responsible for linking incoming sensory information with that which was previously received and stored in memory. In addition, they allow you to compare information that comes from different receptors. The response to the signal is formed in the associative zone and transmitted to the motor zone. Thus, each associative area is responsible for the processes of memory, learning and thinking . Large association zones are located next to the corresponding functional sensory zones. For example, any associative visual function is controlled by the visual associative area, which is located next to the sensory visual area.
Establishing patterns of brain function, analyzing its local disorders and checking its activity is carried out by the science of neuropsychology, which is at the intersection of neurobiology, psychology, psychiatry and computer science.
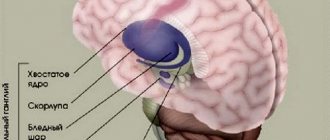
Other structures located in the cerebral hemispheres
Arteries
The brain contains arteries to supply the brain with blood, which are divided into anterior, middle and posterior branches. Each branch helps supply blood to different areas of the hemisphere.
Olfactory bulb
The olfactory bulb, located under the frontal lobe, delivers information directly to the cerebral cortex for interpretation.
Amygdala
The amygdala is a major component of the limbic system. It controls automatic reactions such as the fight or flight response.
Hippocampus
A structure within the temporal lobe, the hippocampus plays a role in learning and memory.
Symptoms of the lesion
Symptoms of the lesion are revealed in such a way that the selected functions are no longer adequately performed. The main thing is not to confuse some symptoms with laziness or imposed thoughts on this matter, although this is part of frontal lobe diseases.
- Uncontrollable grasping reflexes (Schuster reflex)
- Uncontrolled grasping reflexes when the skin of the hand is irritated at the base of the fingers (Yanishevsky-Bekhterev Reflex)
- Extension of the toes due to irritation of the skin of the foot (Hermann's sign)
- Maintaining an awkward arm position (Barre's sign)
- Constantly rubbing your nose (Duff's sign)
- Speech Impairment
- Loss of motivation
- Inability to concentrate
- Memory impairment
The following injuries and illnesses may cause these symptoms:
- Alzheimer's disease
- Frontotemporal dementia
- Traumatic brain injuries
- Strokes
- Oncological diseases
With such diseases and symptoms, a person may not be recognizable. A person may lose motivation, and his sense of defining personal boundaries becomes blurred. Impulsive behavior associated with the satisfaction of biological needs is possible. Because disruption of the frontal lobes (inhibitory) opens the boundaries to biological behavior controlled by the limbic system.
Brain functions
The cerebral hemispheres contain four main lobes, and each lobe performs a different set of functions. Although the brain controls many functions in the body, it is mainly related to the function of each individual lobe and the interaction between them. The brain controls all voluntary actions and is responsible for:
- sensory processing
- emotional control
- motion control
- problem solving
- for language and speech
- visual information
- spatial information
- imagination
- creativity
- musical interpretation
Areas of the brain are responsible for perceiving and interpreting much of the physical world around the body.
Frontal lobe function
- speech
- behavior and personality
- emotions
- body movements
- intelligence and self-awareness
Parietal lobe
- use of language and symbols
- visual perception
- sensation of touch, pressure and pain
- making meaning of signals from other sensory information
Temporal lobe
- memory
- hearing
- language understanding
- organization
- occipital lobe
- light
- color
- movement
- spatial orientation
Insula
- homeostasis
- compassion and empathy
- introspection
- cognitive function
- social experience
Damage to the cerebral hemispheres
Since the cerebral hemispheres control all voluntary actions, damage to this area can lead to a variety of consequences.
Essentially, any condition that affects the brain can cause dysfunction in one or more areas of the brain.
The type and extent of damage will depend on its severity and where in the brain it occurs. For example, damage from an ischemic stroke can occur anywhere in the brain and cause long-term dysfunction in that area.
Other causes of brain damage include accidents, injuries, or other chronic problems that cause atrophy or damage to brain tissue.
Treatment of frontal lobe damage
Treatment for frontal lobe damage is aimed at eliminating the cause of the injury. Your doctor may prescribe medications for an infection, perform surgery, or prescribe medications to reduce your risk of stroke.
Depending on the cause of the injury, treatment is prescribed that may help. For example, if a frontal injury occurs after a stroke, it is important to adopt a healthy diet and physical activity to reduce the risk of future stroke.
The drugs may be useful for people who have problems with attention and motivation.
Treatment of frontal lobe injuries requires ongoing care. Recovery from injury is often a lengthy process. Progress can come suddenly and cannot be completely predicted. Recovery is closely related to supportive care and a healthy lifestyle.