Many diseases in neurological and ENT practice are accompanied by dizziness. Often, a person’s quality of life is significantly reduced. At the same time, the issues of non-drug treatment of dizziness, approaches to vestibular rehabilitation, namely the methods of vestibular gymnastics, are practically not covered. You also need to understand that vestibular gymnastics for dizziness has a significant role, because medications aimed at curing dizziness often do not help immediately and only for a certain period of time, while gymnastics begins to work almost immediately and has practically no contraindications.
Vestibular gymnastics is based on the principle of habituation - “accustoming” the brain to unpleasant stimuli, further allowing them to be ignored. Gymnastics also allows a person to learn to live in conditions of dizziness, improves the quality of life (by normalizing gait, improving the sense of balance), and reduces the risk of falls and injuries. Gymnastics complexes for dizziness should include several types of exercises.
Before performing exercises, you should make sure that there are no folds on the carpets or that there are no foreign objects that could lead to a fall. Exercises should be done in sufficient lighting; it is advisable to have an assistant, who can be a relative of the patient or a caring nurse.
What is the vestibular apparatus?
Exercises for the vestibular apparatus for dizziness should be performed only with the consent of the attending physician. Otherwise, an incorrectly selected load can aggravate the condition of this organ.
The vestibular apparatus is an internal system of the human body, consisting of 3 channels, which in their shape resemble semicircles. Inside them there is a liquid that exerts pressure on the elastic membrane.
This organ determines the acceleration that occurs during any movement of the head (tilts, turns, rotations, and so on). The vestibular apparatus is one of the most complex systems of the inner ear.
Its functioning is to transmit two types of signals to the brain:
- static (occur when the position of the human body changes);
- dynamic (occur when the human body accelerates).
Violations of the vestibular apparatus in the vast majority of cases occur due to:
- serious skull or brain injuries;
- neuritis that occurs as a complication of a viral or bacterial disease;
- diseases of the inner ear (for example, otitis media);
- benign or malignant tumor;
- cerebral circulatory disorders;
- accumulated fluid in the labyrinthine cavity;
- diagnosed sclerosis;
- cerebral infarction or pre-infarction condition;
- chronic stress;
- blood clotting disorders;
- frequent epileptic seizures.
Benign paroxysmal positional vertigo (BPPV)
Benign paroxysmal positional vertigo (BPPV) is a pathological condition of vestibular origin, which is characterized by paroxysmal manifestations of dizziness.
This state is provoked by changes in the spatial position of the human body.
The differences between this type of dizziness are the relative ease of treatment and the possibility of self-improvement.
Etiological factors in the development of functional dizziness (causes)
Benign paroxysmal positional vertigo (BPPV), a very complex condition in etiology, in some cases it is not possible to establish the true cause of the disease.
The most common causes of BPPV include:
- traumatic injuries of the skull and concussions;
- inflammatory processes in the labyrinth of the inner ear;
- undergone surgical interventions in the head area.
Features of symptomatic manifestations
Symptomatically, benign paroxysmal vertigo manifests itself in the form of a feeling that objects around are rotating, this feeling appears after a sudden change in body position.
Paroxysmal dizziness usually manifests itself in the morning after sleep; it is difficult for a person to navigate in space after getting out of bed.
The duration of the paroxysmal period is, as a rule, no more than three minutes, then it goes away on its own without the use of auxiliary techniques.
Additionally, benign paroxysmal positional vertigo manifests itself in the form of dyspeptic disorders, which is a common symptomatic component for all types of vertigo.
An important aspect in diagnosing the disease is that benign positional vertigo is not accompanied by syndromes of organic disorders of the nervous system.
With this pathology, no pathologies develop in the organs of hearing, vision or smell. Thus, the disease does not pose a particular threat to human life, but causes some discomfort.
Diagnostic measures
To make a definitive diagnosis of benign paroxysmal positional vertigo, specially developed Dix-Hallpike functional diagnostic tests are used.
The Dix-Hallpike test is a targeted technique used to diagnose the disease.
To carry out this test, the doctor lays the patient down on the bed, then takes the head with both hands and rotates it in front to the sides around then, holding the head, lays it on the bed. After the exercise, the doctor should ask how the patient is feeling.
Usually, people who have benign positional vertigo are convinced by doctors that dizziness after such a shake is a normal condition for them.
Objectively, a patient has nystagmus that is directed toward the floor, to the side or to the top; this depends on the direct localization of the pathological process in the semicircular canals of the inner ear.
In case of a negative effect, the exercise should be repeated a few minutes after rest. Sometimes it happens that after conducting a diagnostic test in a supine position, a positive result cannot be achieved, but the condition manifests itself after the patient gets up from the couch and the body acquires a sitting position.
When repeating positional tests, the severity of the results as a rule decreases somewhat; this also must be taken into account when making a diagnosis. As an addition to the positional test, you can use not only rotation towards the head, but also the entire body.
The most difficult for patients to tolerate is a change in body position from lying to standing.
Instrumental studies
As an instrumental diagnosis of the disease, methods are used to assess the severity of nystagmus; for this purpose, methods such as electrooculography and videooculography are used.
In order to exclude organic pathology from the central nervous system or oncological pathology, patients must undergo magnetic resonance imaging of the brain. To exclude pathology from otolaryngology, it is necessary to undergo a consultative examination with an appropriate specialist.
Differential diagnosis of benign positional paroxysmal vertigo
Unlike tumor-like formations in the brain, as well as pathologies of the posterior cranial fossa, with the benign development of vertigo, there are no signs of damage to the sympathetic and parasympathetic nervous system; common signs are symptoms of impaired balance and positional vertigo.
Repeated positional functional testing for ordinary dizziness is usually characterized by a decrease in the severity of the positive result, since in organic pathology, repeated testing does not affect the severity of the result.
Nystagmus of a positional nature can also manifest itself in a disease such as multiple sclerosis or acute cerebrovascular accident, while all the symptoms of damage to the nervous system remain.
Therapeutic measures to eliminate pathology and discomfort
Conservative treatment without the use of drugs includes the following methods:
Brandt-Daroff method
The patient can perform this exercise independently at home.
To carry out this technique, the patient needs to sit in the center of the bed and bend several times from side to side. Then the patient is injected back into a horizontal position and repeats the movements in a supine position.
It is necessary to rest the body for a minute, then repeat the indicated Brandt Daroff exercises.
The method for treating the disease is repeated three times throughout the day. The duration of the procedure is determined individually depending on the general well-being of the patient.
Semont maneuver
This technique can be performed either independently or with the help of a qualified specialist.
The patient sits on the bed, the doctor takes the patient's head with both hands and turns it sharply, then injects it on the same side without changing the position of the head relative to the original plane.
The patient should lie down until all discomfort disappears.
After rest, without changing the fixed position of the patient’s head, the patient is returned to a sitting position, the head is turned and placed on the opposite side, the patient should also rest. This exercise is repeated 2-3 times, once a day.
In cases where a patient suffering from benign paroxysmal vertigo has a life history of pathologies from the cardiovascular system, cardiac tonic drugs are administered before the procedure as a specific predication.
If nausea and vomiting occur during the procedure, patients are prescribed antiemetic drugs.
Epley maneuver
A procedure of this nature is carried out only by qualified specialists. The peculiarity of this method is that the procedure is carried out using smooth and slow body movements.
The patient should initially sit on the couch, the doctor takes the head with both hands and fixes the head, turning it to the side in the same position, the patient’s head is placed on his back. After this, the person’s body is turned over on its side, and then slowly seated in its original position.
This method of non-drug treatment is very effective and in most cases, repeating two or three sessions can help completely get rid of the pathological condition.
The effectiveness of this method depends entirely on how professional the specialist performing this procedure is.
Lempert maneuver
This technique is carried out exclusively by a qualified specialist. The initial position of the patient should be sitting along the couch. Turning the head forty-five degrees, fix it in the plane of the horizontal body on the side of the focus of the pathological condition.
After this, the patient is placed in a supine position on his back and the position of the head is slowly changed in the opposite direction, then the head is turned to the other side and the position of the body is changed from back to stomach, while the head should rotate together with the human body.
The exercise can be repeated several times, but with the condition of maintaining a rest period.
Surgical technique for treating the disease
Surgical intervention is performed in cases where conservative treatment of the disease has shown absolutely no positive results.
This treatment method is carried out very rarely and in quite exceptional cases.
For this purpose, surgical intervention techniques such as:
- filling the lumen of the semicircular bony canal of the inner ear with fragments from the bone structure, which is taken from another part of the skeleton of the human body. The most optimal bone for transplantation is the tibia;
- selective removal of nerve endings that innervate the vestibular canals of the human inner ear;
- total removal of structures and spongy substance of the bone labyrinth;
- destructive destruction of labyrinth structures using specially selected laser installations.
Absolutely all surgical methods are extremely traumatic for humans and therefore should be performed only for special medical indications.
After surgery, the patient must undergo antibacterial therapy in order to prevent the development of complications of an infectious nature.
To prevent dysentery as a side effect of antibiotics, the patient is prescribed probiotics in combination.
Disease prevention
Preventive measures for benign positional paroxysmal vertigo have not been developed to date since the etiological factors in the development of the disease have not been fully elucidated.
As a recommendation, patients should not drive a car for some time.
The pathological condition may persist for several days or weeks after treatment. As for the restoration of ability to work, it can also be difficult for several weeks, but one should take into account the fact that benign positional vertigo can recur over time and when such a moment occurs is not known.
Forecast
The prognosis for recovery is usually favorable; this condition does not pose a particular danger to the patient’s life. Depending on what disease or injury could have triggered the development of this condition, further recovery and the effect of the treatment will depend.
The prognosis for full recovery also depends on how promptly the patient sought qualified medical help.
The danger of this disease lies in the fact that it is quite difficult to carry out diagnostic measures, and if the disease is provoked by an infectious disease of the inner ear, when the infectious process is advanced, the infection can spread into the cranial cavity and lead to death for the patient.
posts on the topic
Source: https://tvojajbolit.ru/nevrologiya/dobrokachestvennoe-paroksizmalnoe-pozitsionnoe-golovokruzhenie-dppg-chto-eto-takoe-simptomyi-i-lechenie/
Benefits of vestibular exercises
The main advantages of vestibular gymnastics include:
- reducing the frequency and intensity of dizziness (if the vestibular apparatus is malfunctioning, a person begins to feel dizzy at least 2-3 times a day);
- minimizing the number of fainting and pre-fainting states;
- improving balance skills;
- decreased sweating;
- normalization of the condition of the eyeballs (if there are disturbances in the functioning of the vestibular apparatus, the eyeballs may begin to tremble, which will significantly affect the quality and acuity of a person’s vision);
- improved vision (first of all, gaze focusing improves);
- eliminating fog before the eyes;
- normalization of speech (difficulties in pronouncing some nasal sounds are eliminated);
- normalization of movement coordination;
- normalization of the respiratory system;
- elimination of surges in blood pressure (they become especially noticeable in people with diagnosed hypertension of degrees 2 and 3);
- normalization of body temperature (if there are disturbances in the functioning of the vestibular apparatus, body temperature usually decreases);
- evening out the tone of the skin on the face and décolleté (if there are disturbances in the functioning of the vestibular apparatus, a person’s skin acquires a pale tint).
Indications for use
Brandt-Daroff vestibular gymnastics helps to concentrate attention, but does not train muscles. This type of exercise is recommended for use by all people, including the elderly, who suffer from frequent attacks of dizziness.
This set of exercises is shown to people:
- those who have had a stroke;
- those suffering from BPPV;
- with general impaired coordination of movements;
- with osteochondrosis;
- with high numbers on the tonometer;
- with chronic migraine;
- with mental disorders;
- with lung pathologies
- with minor and serious spinal injuries;
- with dyscyclic encephalopathy;
- having pathologies affecting the ear areas.
Brandt-Daroff vestibular exercises are also recommended for people who have suffered a history of brain injury.
Contraindications
Exercises for the vestibular system for dizziness are contraindicated in people with:
- progressive serious disease of the vestibular apparatus;
- other diagnosed diseases accompanied by frequent dizziness;
- perilymphatic fistula;
- diagnosed benign and malignant neoplasms localized in the brain;
- epilepsy.
If you have one or more symptoms of contraindications from the list above, you should consult your doctor before starting vestibular gymnastics.
Indications for classes
Dizziness in rare cases becomes a reason to go to the hospital. But do not underestimate the malaise, because in some cases it is an alarming signal, warning about the likelihood of developing a serious illness.
Indications for vestibular gymnastics include diseases such as the post-stroke period, osteochondrosis, pathologies of the ear area, as well as conditions after traumatic brain injury.
But it’s not always possible to do gymnastics yourself.
Self-medication can worsen the patient's condition when he has ischemic brain damage , and there is also a high likelihood of compression of the vertebral artery.
Only the doctor should decide whether gymnastics is indicated for the patient and in what way he can do it, independently or with the help of a doctor. Do not self-medicate and consult a specialist!
Basic rules of training
Among the basic rules for training the vestibular apparatus:
- Exercises must be performed daily, at least 2 times a day (otherwise the exercises will be ineffective);
- In terms of time, such charging should last at least 20-30 minutes. followed by rest (after a break of 10-15 minutes, it is permissible to continue doing the exercises. Otherwise, in the absence of rest, overtraining of the vestibular apparatus may occur);
- if, according to the technique of performing exercises, a person needs to stand, he should sit in this position without shoes and socks or, when exercising outdoors, in comfortable flat-soled shoes without heels;
- the pace of performing exercises to train the vestibular apparatus should be slow (otherwise the condition of the organ in question can be aggravated);
- It is not recommended to perform exercises during exacerbation of other diseases, regardless of whether they are seasonal (for example, ARVI) or chronic;
- It is recommended to schedule consultations with the doctor monitoring the patient’s condition so that they occur at least once every 7-14 days (this is necessary for timely adjustment of the training program in the absence of results or aggravation of the person’s condition).
Purpose
Correction and training of the vestibular apparatus is a fairly important part of therapy and training in human coordination. Today, there are quite a large number of methods for correcting the vestibular apparatus, among which the leading place is occupied by vestibular gymnastics for dizziness, which not only improves the functioning of the victim’s body, but also helps him avoid falls and other side effects from the pathology.
Vestibular gymnastics is a set of exercises and tasks that the patient performs for a certain time and at a certain interval, allowing:
- if necessary, monitor the pathology of the vestibular apparatus;
- reduce the likelihood of injury if you fall from dizziness;
- quickly adapt to the patient’s new location and new conditions;
- reduce or completely eliminate the manifestations of pathology - dizziness, nausea;
- it is easier to endure long trips and other difficulties;
- increase blood flow to the brain organs, thereby increasing its saturation with oxygen;
- improve the quality of life after neurological diseases;
- improve vision clarity;
- train the patient's balance.
Vestibular gymnastics has a particularly good effect for older people who, due to age and illness, lose the normal ability to correctly navigate in space and maintain balance.
Exercise for adults
Exercises for the vestibular system for dizziness can be performed standing or sitting, using various organs.
For eyes
The most effective exercises for the vestibular system involving the eyes are:
| Exercises for the vestibular apparatus | Brief description of the technique |
| Moving the eyes left and right | 1. Sit on a chair, taking a comfortable body position. 2. In your hands, at a distance of 30 cm from your face at eye level, fix a small sheet of paper that should not be visible. Several phrases should be printed on the sheet in a regular medium-sized font. 3. Move the sheet of paper to the right as slowly as possible, fixing your gaze on its surface. 4. Move your gaze to the left along with the piece of paper you are using. 5. Repeat the steps described in steps 3 – 4, moving the sheet of paper up and down. The head must remain motionless while moving the sheet. By regularly performing this exercise, a person will begin to maintain focus on what is written, regardless of whether the paper is in motion or fixed in one position. |
| Moving your finger in front of your face | 1. Take a comfortable body position. 2. Place your straight index finger in front of your eyes at a distance of 20-30 cm. Fix your gaze on your finger. 3. Slowly move your finger forward without losing focus. Without pausing in the far position, return your hand to its original position. 4. Perform the actions described in paragraph 3 for 30 – 90 seconds. |
For the head
The most effective exercises for the vestibular system that involve the head are:
| Exercises for the vestibular apparatus | Brief description of the technique |
| Head tilts in different directions | 1. Sit in a comfortable position, sitting or standing, place your hands on your belt, spread your legs shoulder-width apart. 2. Fixing your gaze at one point, tilt your head to the right. 3. Without pausing, move your head as far to the left as possible. When bending, you need to feel the maximum stretch of the neck muscles; It is not recommended to move your eyes. 4. Tilt your head forward and back. Perform the exercise for 15-30 seconds. |
| Rotate your head left and right | 1. Take a comfortable body position; straighten your back; lengthen the neck; Place your arms and legs in a comfortable body position. 2. Draw a semicircle in the air in front. 3. Without pausing at the extreme points, draw a semicircle in the air in the opposite direction. 4. Repeat the steps described in paragraphs 2-3, performing rotations while throwing your head back. The pace of head rotations must be determined as follows: 2-3 rotations in front and behind at a fast pace; 2-3 rotations front and back at a slow pace. Repeat the above steps for 2-3 minutes. |
Standing
The most effective exercises aimed at normalizing the functioning of the vestibular apparatus, performed from a standing position, are recognized:
| Exercises for the vestibular apparatus | Brief description of the technique |
| Changing body position | 1. Stand up straight, placing a chair with stable legs at a distance of 5-10 cm. 2. Direct your gaze straight ahead. 3. Take a deep breath, then slowly lower yourself onto the chair. The back should remain straight while changing position. 4. Without pausing, stand in front of the chair, returning to the starting position. 5. Repeat changing body position for 30-60 seconds, while keeping your eyes wide open. |
| With a ball | 1. Stand up straight; artificially stretch the neck; Place your feet shoulder-width apart. 2. Hold a small ball in your hands, the size of which should not exceed the diameter of a tennis ball. 3. Throw the ball from one hand to the other for 1-3 minutes, watching the movement of the object with your eyes. The ball should pass just above eye level. The body and head must remain motionless while moving the object. |
| Changing position with rotation | 1. Stand up straight, placing a chair with stable legs at a distance of 5-10 cm. 2. Direct your gaze straight ahead. 3. Rotate around your axis, and then slowly lower yourself onto the chair. 4. Take a deep breath, then, returning to the starting position, repeat the steps described in step 3. The optimal time for performing the exercise is 60 seconds. |
Exercises for children
Exercises for the vestibular system for dizziness must be selected taking into account the age of the individual. For young children, the most effective loads are:
| Exercises for the vestibular apparatus | Brief description of the technique |
| Rotations from a lying position | 1. Place the child on a flat surface on his back. 2. By lightly pulling the baby’s legs, provoke his reflex to roll over onto his stomach. 3. Without pausing, pull the legs again, thus turning the baby onto his back. 4. Repeat the above steps 5-10 times for each side. |
| Swinging on a fitball | 1. Place the baby on the fitball, placing his stomach on the ball. 2. Holding the child with your hands, perform rocking movements to the right, left, forward and back. 3. It is recommended to perform the exercise for 3-5 minutes. |
| Rocking on your knees | 1. Place the child on the adult’s lap with his stomach down. 2. Holding the baby’s body, as well as his head, alternately tear off the heels of the right and left legs. 3. The exercise should be performed for no more than 30 seconds. at a slow pace, observing the child’s emotions. After the specified time has passed, take a short break (5-10 seconds), and then perform another approach. When performing this exercise, the baby not only improves the functioning of the vestibular apparatus, but also stimulates the release of gases. |
Gymnastics for dizziness
The most effective vestibular gymnastics exercises aimed at eliminating dizziness are recognized:
Brandt-Daroff vestibular gymnastics - effective exercises for the vestibular system for dizziness
| Exercises for the vestibular apparatus | Brief description of the technique |
| Option 1 | 1. Sit on a bed or sofa, straightening your back as much as possible. Hands must be placed in any position, legs pressed firmly to the floor. 2. Slowly lie on your left side, while leaving your head elevated 45 degrees. To quickly orient yourself in space, you need to imagine that your gaze is fixed on a person located at a distance of 1-1.5 m. 3. Fix the position for 30-45 seconds. 4. Slowly return to the starting position, sitting again on the bed. 5. Repeat the steps described in paragraphs 2-4, while lying on the opposite (in this case, right) side. 6. The above exercise must be performed at least 5 times for each side. |
| Option 2 | 1. Sit on a bed or sofa, straightening your spine as much as possible. 2. Turn your head to the right, then maintain the position for 30 seconds. 3. Lie on your left side, while throwing your head back at an angle of 45 degrees. 4. After 30 seconds in this position, slowly return to the original position. 5. Repeat the steps described in paragraphs 2-4, performing the exercise in a mirror manner. 6. The optimal time for performing the exercise is 2-3 minutes. |
DPP - what is it, causes, sand in the ear, treatment options
Benign paroxysmal positional vertigo is more often referred to simply as BPPV. So in short. For patients, another name for the pathology is known - “sand in the ear.” Yes, it feels that way.
This sensation is given by the internal structure of the inner ear, which is part of the vestibular apparatus and is responsible, among other things, for positioning the body in space and preventing parasitic dizziness.
Let us focus on the fact that dizziness . It's not permanent. It appears occasionally when the position of the head changes.
BPPV is a common pathology. Up to 17% of all cases of dizziness are associated with this disease. This problem occurs more often in women than in men.
DPP - what is it?
BPPV is, as stated above, an abbreviation for the term “benign paroxysmal positional vertigo.” An attack of this type of dizziness is associated with a change in the position in space of the body and head. However, it differs from, for example, orthostatic collapse in the duration and condition after the attack.
For reference. That is, BPPV is a short-term vestibular disorder observed when turning the head.
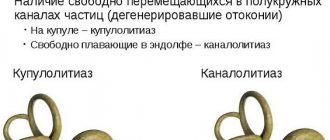
It is accompanied by nausea, and in some cases, vomiting. The cause of the pathology is the presence of freely floating otoliths (crystallized calcium bicarbonate) in the endolymph. Their displacement causes irritation of the ciliated cells and, accordingly, dizziness.
For diagnostic purposes, special tests are used, and for therapeutic purposes, vestibular gymnastics, Epley and Semont maneuvers are used. The effectiveness of drug therapy has not been proven, so prescribing medications is advisable only as an adjunct.
DPP - causes
To imagine the mechanism of development of an attack of dizziness with BPPV, you should familiarize yourself with the structure of the vestibular apparatus.
It consists of the superior, posterior and horizontal semicircular canals with extensions (ampoules), as well as a pair of sacs - oval and round. All these structures, forming the so-called labyrinth, are filled with endolymph and contain accumulations of sensitive ciliated cells.
In the ampoules, the receptor cells are covered with gelatinous caps - the cupula, and in the channels - with a special membrane with inclusions of crystallized calcium.
The main cause of so-called benign positional vertigo or otolithiasis is a disorder of metabolic processes in the inner ear. By the way, otolithiasis is another name for BPPV.
Normally, these crystals (otoliths or otoconia) are localized in the membrane, and there is a constant dissolution of old formations and their replacement by new ones.
If production increases or their utilization slows down, undissolved otoliths move freely in the endolymph, periodically causing malfunctions of the vestibular apparatus.
Typically, otoconia accumulate in the lumen of the posterior semicircular canal or ampoules, sticking to the cupula. During movement, they irritate the hair cells directly or dislodge their jelly-like covering.
For reference. As a result, the perception of angular accelerations is disrupted, and a short-term attack of dizziness occurs. When the movement of the otoliths stops and they settle to the bottom of the canal (they stop moving the cupula), the head stops spinning.
Factors that disrupt the process of formation and dissolution of otoconia are:
- TBI leading to damage to the otolithic membrane;
- viral inflammation of the labyrinth of the inner ear;
- Meniere's disease;
- taking antibiotics that have an ototoxic effect (Gentamicin and other aminoglycosides);
- spasm of the artery supplying the vestibular apparatus with blood;
- surgical operations.
In accordance with the localization of free otoliths, otolithiasis is divided into two types. The accumulation of crystallized calcium in the channels is called canalolithiasis, in the ampoules - cupulolithiasis. The disease is called benign because it is caused by mechanical irritation, and not by organic damage to the structures of the inner ear.
DPP - symptoms
The main symptoms of BPPV include the following:
- rotational vertigo,
- short duration (paroxysmal): dizziness lasts seconds or minutes,
- Nausea and vomiting are sometimes recorded.
Benign paroxysmal positional vertigo begins when the head is thrown back or turned, since such movements provoke movement of the otoliths. The attack most often occurs when the body is in a horizontal position, so patients usually complain of morning dizziness associated with turning over in bed.
Why dizziness occurs, causes and types
Night attacks lead to awakening.
For reference. Subjectively, paroxysm, which is the main symptom of BPPV, is felt as rotation of surrounding objects in different planes.
The duration of an individual attack is on average half a minute, but it is perceived as longer (about 5 minutes). The frequency of occurrence during an exacerbation period varies from weekly repetition to several paroxysms per day.
In some cases, BPPV attacks are isolated. Remissions, as a rule, last a long time, amounting to months and even years.
There are no additional signs of vestibular disorders such as hearing loss or hearing loss, headache, or tinnitus in benign paroxysmal positional vertigo.
Attacks may only be accompanied by nausea or, less commonly, vomiting. In the intervals between them or after a single paroxysm, patients note symptoms characteristic of dizziness of a non-systemic nature.
There are sensations of instability, swaying, and so-called “lightheadedness.”
BPPV in itself does not pose a danger to human health and life, has no negative consequences, and the prognosis of the disease is favorable. However, if the attack occurs in conditions that require fine-tuned coordination or increased concentration, an accident is likely.
For example, while driving a car or working at height. In addition, frequent exacerbations negatively affect the patient’s psycho-emotional state. The result can be depression, hypochondria, and neuroses.
Diagnosis of BPPV
When contacting a neurologist, a medical history is taken and a series of specific tests are performed. The diagnosis of benign paroxysmal positional vertigo is made primarily on the basis of clinical data. To confirm it, the doctor performs the Dix-Hallpike test.
The person being tested, sitting on the couch and turning his head to the affected side (the angle of rotation should be 45⁰), fixes his gaze on the bridge of the nose of the person conducting the test. Then you quickly need to lay him down on his back so that the fixed head hangs down slightly.
After 20 seconds, return to its original state, repeat on the other side and evaluate the result:
- If after 1-5 seconds in a lying position the patient becomes dizzy and rotatory nystagmus (rotation of the eyeballs) occurs, BPPV is diagnosed. When returning to the starting position, the eyes move in the opposite direction.
- The absence of both symptoms indicates that the test is negative.
- A positive bilateral result indicates a traumatic origin of the pathology.
- Dizziness without nystagmus is confirmation of the diagnosis, but with the prefix “subjective”.
If the test is repeated several times in a row, the accumulation of otoliths that irritate the ciliated cells will dissipate. Accordingly, the head will no longer feel dizzy when tilted, and the nystagmus will be exhausted.
To fix the latter during diagnostics, special techniques are used. Electronystagmography or videooculography.
Recording equipment is needed because eye movements during the Dix-Hallpike test cannot always be recorded visually.
For reference. To further confirm benign paroxysmal positional vertigo, a so-called rotation test is performed.
The patient, lying on his back, throws his head back at an angle of 30⁰. The doctor sharply turns it to the affected side and observes the horizontal nystagmus that occurs after a short latent interval.
By the nature, speed and direction of movement of the eyeballs, one can determine the localization of otoliths, and in the case of canalolithiasis, in which particular canal the accumulation of otoliths is located.
The main symptoms of BPPV are characteristic of some other vestibular disorders, diseases of the nervous and cardiovascular systems.
Differential diagnosis is required if vestibular neuronitis, multiple sclerosis, Meniere's disease, arterial hypotension, Barré-Lieu and vertebral artery syndromes are suspected.
With these pathologies, in addition to dizziness, hearing loss, neurological disorders, tinnitus, cephalalgia, and neck pain are also observed.
DPP - treatment
Therapy used for BPPV is predominantly conservative. Surgical intervention is a radical measure, fraught with complications and advisable only if there is no effect from other methods.
For reference. The basis of treatment is various techniques that allow you to move otoliths in the labyrinth and stop exacerbations of the disease, as well as performing special Brandt-Daroff gymnastics.
Taking medications is indicated only in the acute phase of the disease and has the nature of an adjunct.
How to get rid of dizziness - what to do
Epley maneuver
This method, by sequentially changing the position of the head in space, allows the otoconia to be moved from the semicircular canals to one of the sacs.
It is used for canalolithiasis to eliminate the cause of dizziness – irritation of the ciliated cells.
It goes like this:
- Turning the head towards the problematic ear by 45⁰, the patient lies on his back from a sitting position. The head must hang over the edge of the couch, and it must be fixed in this way for a minute and a half.
- Then turn 90⁰ in the other direction, simultaneously turning over from your back to the same side.
- Then the face turns towards the floor for a while.
- The technique is completed by moving to the initial sitting position, but with the head lowered to the chin.
For reference. This sequence of manipulations allows you to change the orientation of the labyrinth in space and gradually move the otoliths into the sac from the posterior semicircular canal.
Semont's reception
In case of cupulolithiasis, the ampoules of the labyrinth must be freed from otoconia. For this purpose, another technique is used.
Sitting on the couch with his legs down, the patient must fix his head turning towards the healthy ear and not change its position the entire time the technique is being performed.
First, the doctor abruptly places the person on the affected side, then returns to the previous position and lies down on the other side.
Correct, quick execution helps to free the cupula from crystals adhering to it.
Vestibular gymnastics
If the diagnosis is confirmed, you should regularly perform a set of Brandt-Daroff exercises.
It is performed in the morning, after waking up, and consists of the following sequence of movements:
- sit across the bed with your feet on the floor;
- turn your head to the left (rotation angle is about 45⁰);
- without changing its position, lie on your right side;
- lie there for half a minute or until the dizziness disappears;
- return to original position;
- repeat for the other side.
You need to repeat the complex daily, and if you have dizziness, several times a day.
Surgery
For reference. The Semont maneuver, the Epley maneuver used for dizziness, as well as regular vestibular exercises usually provide the required therapeutic effect, which allows you to get rid of BPPV paroxysms for a long time.
But in some cases, conservative therapy is ineffective, and surgery is prescribed.
Surgical intervention is carried out taking into account the severity of the pathology, the age characteristics of the patient using various techniques. So, you can fill the semicircular canal, which contains clusters of otoliths, or cross some vestibular fibers.
Sometimes complete removal of the labyrinth is indicated, which is carried out using laser destruction.
Drug therapy
Many experts doubt the advisability of using medications. Medicines used for BPPV are not able to eliminate the causes of dizziness, but only alleviate the symptoms of the disease during acute periods.
The basis of treatment consists of techniques and gymnastics that dispel clusters of otoconia. However, an otolaryngologist may recommend tablets that improve cerebral circulation and metabolic processes in brain tissue as a supplement.
For reference. Such drugs as Betahistine, Cinnarizine, and products based on the gingko biloba plant are considered quite effective and safe.
Conclusion
Vestibular disorder, caused by the movement of free otoliths in the canals and ampullae of the labyrinth of the inner ear, is considered an age-related disease. The majority of patients who consult a doctor with characteristic complaints are people aged 70 to 78 years.
For reference. The slowdown of metabolic processes, characteristic of older people, is the main reason for the excess amount of crystallized calcium in the vestibular apparatus. The proportion of young patients with this diagnosis is insignificant.
Only an otolaryngologist or neurologist can recognize the symptoms characteristic of BPPV and prescribe treatment; differential diagnosis is also necessary. Typically, conservative non-drug therapy methods provide positive results in the form of relief of dizziness attacks and long-term remission.
Pathology is treated surgically only in exceptional cases when its manifestations cannot be eliminated by other methods. Medicines are used only as an additional remedy during an exacerbation.
Source: https://neuromed.online/chto-takoe-dppg/
For osteochondrosis
Exercises that normalize the functioning of the vestibular apparatus for osteochondrosis can also help get rid of dizziness and other unpleasant manifestations of the disease:
| Exercises for the vestibular apparatus | Brief description of the technique |
| Neck stretch | 1. Stand up straight; put your hands on your belt or place them in a free position along the body; place your feet shoulder-width apart. 2. As you exhale, stretch your neck forward as much as possible, while feeling the stretching of its back surface. 3. Lower your head down as smoothly and slowly as possible, without changing the initial degree of neck elongation. 4. Feeling a stretch in your neck and upper back, hold the position for 20 seconds. 5. With a deep breath, slowly return to the starting position, moving your neck in the opposite direction along a similar route. 6. The optimal time for performing the exercise is 2-3 minutes. |
| Forward bends | 1. Stand up straight; place your feet shoulder-width apart; bring your arms in front of you at chest level, then cross them without changing the distance between them and the floor; stretch your neck. 2. With a deep exhalation, move your arms forward, while slightly moving your body in the same direction. 3. Feeling the maximum stretch in your neck and upper back, fix the position for as long as possible (at least 30 seconds). 4. Inhaling deeply, take the starting position. |
Complex for rehabilitation after stroke
Some of the simplest but most effective exercises included in the rehabilitation complex after a stroke are:
| Exercises for the vestibular apparatus | Brief description of the technique |
| Shoulder rotations | 1. Sit on a stable surface; press your feet to the floor; place your legs in a free position; straighten your back. 2. Perform 5 rotational movements with your shoulders forward at a slow pace. The joints should rise slightly. 3. Complete the exercise in the uppermost position of the shoulders, and then perform similar movements in the opposite direction. 4. The optimal time for performing the exercise is 1-2 minutes. If a person experiences dizziness while performing the exercise, the recommended load time should be divided by inserting breaks of 5-10 seconds between the main approaches. |
| Body turns | 1. Sit on a stable, flat surface; press your feet to the floor, placing your feet shoulder-width apart; lower your arms down and leave them in a free position. 2. Take a deep breath and then slowly turn to the right. The body should be rotated until discomfort and severe muscle tension occur. 3. As you exhale, you must return to the starting position. 4. Perform a similar turn in the other direction. 5. After 2-3 turns in each direction, it is recommended to gradually increase the pace of movement until it is comfortable for a particular person (the maximum load should be determined by a doctor who has a complete understanding of the health status of the patient who has suffered a stroke). |
Gymnastics for the elderly
The optimal load options for older people within the framework of vestibular gymnastics are:
| Exercises for the vestibular apparatus | Brief description of the technique |
| Head rotation | 1. Take a comfortable position, sitting or standing. Straighten your back; stretch your neck; lower your arms along your body. 2. As you exhale, begin to slowly lower your head down, while carefully turning it left and right. 3. Having reached the lowest possible point, when the neck muscles are stretched to the maximum (there should be no pain), begin moving the head in the opposite direction, maintaining the original amplitude of turns. 4. The optimal number of repetitions is 10 times in each direction at the slowest pace possible. |
| Diagonal head tilts | 1. Take a comfortable position, sitting or standing. Straighten your back; stretch your neck; lower your arms along your body; press your feet to the floor. 2. Slowly lower your head forward so that the back of your head points diagonally to the right. 3. Without pausing, also at a slow pace, tilt your head diagonally back.
5. Perform the exercise the same number of times in a mirror manner. |
Vestibular exercises performed by older people should be performed under strict blood pressure (BP) control. It is important not just to focus on your own feelings, but also to record blood pressure readings before, after, and, if necessary, during the session.
If the vestibular apparatus does not function properly, a person may experience dizziness. Before starting special exercises to normalize the condition, it is important to determine the cause of the condition in question with the help of a qualified neurologist.
In the absence of serious concomitant diseases, it is necessary to perform vestibular gymnastics on a regular basis, both to eliminate current discomfort (dizziness) and for preventive purposes, thus stimulating local blood supply.
Damage to the lateral semicircular tubule
A lesion of the lateral RCC is detected with the patient lying down by turning the head in the plane of the canal from right to left and vice versa (roll test). Horizontal nystagmus occurs, with a clonic component directed downward, mainly when the affected ear is turned downward; if the healthy ear is located below, nystagmus also occurs, the clonic component of which is directed downward, but less pronounced.
In a quarter of patients, canalolithiasis in the lateral RCC is combined with canaloliasis in the posterior RCC. In contrast to downward-directed nystagmus, the clonic component of evoked nystagmus is directed toward the overlying ear. This form is combined with the location of otoliths in the anterior part of the lateral ACC or the otolith fixed to the cupula, while with freely moving otoliths, nystagmus occurs directed towards the underlying ear.
Test results may be influenced by cervical spinal canal stenosis, radiculopathy of the cervical segments of the spinal cord, severe kyphosis, restrictions of movement in the cervical spine: rheumatoid arthritis, ankylosing spondylitis, Paget's disease, spinal cord injury, morbid obesity, Down syndrome. In this case, it is possible to use a Barany swivel chair.
If the test results are negative, a preliminary diagnosis of BPPV is made based on complaints of positional vertigo and is confirmed by successful performance of vestibular maneuvers.
If examination reveals a nystagmus that differs from that described above, as well as other neurological symptoms, it is necessary to exclude other lesions of the nervous system.
Lying on your side with the affected ear facing up for 12 hours,
Barbecue method
The “barbecue” method - turning the patient 360˚ - the patient in a lying position is successively turned towards the healthy ear by 90˚ until he takes the starting position.
The patient's head is rotated 270˚ from the affected ear to the healthy one.
Special studies have shown the sufficient effectiveness of exercises performed by patients. There were no differences in the effectiveness of the maneuver in specialized clinics and in primary care settings.