Find out more about other diseases starting with the letter “F”: Phakomatoses; Phantom pain; Fibromyalgia; Focal cortical dysplasia; Focal epilepsy; Funicular myelosis.
Phakomatoses are a group of diseases caused by a genetic predisposition, characterized by a progressive course and having polymorphic symptoms, mainly affecting the nervous system and organs of vision. A distinctive symptom is the formation of tumors of internal organs.
The diagnosis is established after consultations with many specialized specialists, as well as on the basis of a comprehensive examination using MRI, CT, ultrasound, ECG, EEG, and ophthalmoscopy. Treatment of phakomatosis is aimed at eliminating symptoms, using psychotherapy and surgical treatment. The prognosis of the disease depends on its form and severity.
general information
At the end of the 19th century, clinical variants of phakomatoses were described by many doctors. In 1923, the Dutch ophthalmologist Van der Hoove proposed combining diseases with combined lesions of the nervous system, internal organs, and eyes, which are accompanied by skin manifestations in the form of hypo- and hyperpigmentation, neurofibroma, and angioma. Van der Hoeve introduced the definition of "phakomatosis".
In modern medicine, “phakomatosis” is not a nosological entity, but belongs to a certain group of diseases. The most common diseases in this nosological group are Recklinghausen's neurofibromatosis and tuberous sclerosis. This group includes almost 30 neurocutaneous syndromes - Louis-Bar, Hippel-Lindau, Bonnet-Dechaumes-Blanc, Sturge-Weber, Ito hypomelanosis, pigment incontinence syndrome.
↑ Sturge-Weber syndrome
Sturge-Weber syndrome is a rare disease involving the nervous system, vision and skin in the pathological process.
In the classic form, the syndrome manifests itself as a purplish-red spot localized on one side of the face in the zone of innervation of the trigeminal nerve. Neurological symptoms of tics include epilepsy, mental retardation and hemniaresis. The main manifestation of the disease in the visual organ is glaucoma. The genetic mechanism of this syndrome is not fully understood. Most authors attribute the disease to a somatic mutation during early fetal development, but there is a point of view that the cause of the disorder is a lethal gene preserved due to mosaicism.
The embryogenesis of the syndrome apparently involves incomplete differentiation of the primary mosenchyme of the vessels of the cranial ectoderm and the underlying neural tube in periods from A to 8 weeks of gestational age. On the other hand, there is an assumption that the defect is the result of a disruption in the communication between the cortical veins and the superior sagittal sinus, which causes the appearance of a malformation of the vessels of the soft and arachnoid membranes of the brain and the formation of collateral circulation.
Diagnostic criteria
for Sturge-Weber syndrome with the classic triad of symptoms
- Neurodermal angiomatosis.
- Angiomatosis of the soft and arachnoid membranes of the brain (Fig. 24.10).
- Pathology of the organ of vision.
- Angpomatosis of the skin.
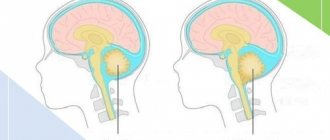
Abortive two-symptomatic form of Sturge-Weber syndrome (Fig. 24.11)
- Angiomatosis of the organ of vision and skin.
- Neurodermal angiomatosis.
Abortive monostomytic form of Sturge-Weber syndrome
- Isolated angiomatosis of the soft and arachnoid membranes of the brain.
- Isolated angiomatosis of the skin in the area of innervation of the trigeminal nerve.
Extended Sturge-Weber syndrome These cases include combinations with other neuroectodermal syndromes:
- Klipnel-Trenaunay-Weber syndrome;
- oculodermal melanosis (nevus of Ota);
- neurofibromatosis;
- tuberous sclerosis;
- Hippel-Lindau disease;
- Wiburn-Mason disease;
- marble leather;
- neurodermal melanosis;
- pigmentovascular phakomatosis type IVa.
Reasons for the development of phakomatosis
Phakomatosis is a genetic disease during which, starting from the early embryonic period, disorders occur in the processes of cell differentiation and development. Pathologies develop preferentially in the ectodermal germ layer, from which nerve fibers, outer layers of skin, nails, hair, retina, and epithelium of the oral and nasal mucosa develop. What remains are cells that have stopped developing and remain at the stage of permanent embryonication. From these tumors begin to form - hamartomas. Tumors of embryonic origin can be localized in different places and accompany phakomatosis of any nature.
Pediatricians and neurologists often define phakomatosis as neurodermal dysplasia, based on data on the pathology of the formation of ectodermal structures. It should be noted that in phakomatosis, ectodermal dysplasia is often combined with pathologies of differentiation of the mesodermal and ectodermal germ layers.
Mesodermal dysplasia leads to the formation of aneurysm, angioma, rhabdomyoma, and bone tissue pathologies. Clinical signs of ectodermal dysplasia include polyps of the gastrointestinal tract - stomach polyps, rectal polyps, intestinal polyps.
The progress of DNA methods and genetics has made it possible to identify genes in which deviations from the norm explain phakomatosis. Genetic changes lead to a decrease in the synthesis of factors responsible for blocking tumorigenesis. This is the most likely reason for the formation of multiple tumors that characterize phakomatoses. Inheritance occurs according to an autosomal dominant trait with incomplete penetrance, which explains the fact that the disease is not recorded in every generation.
Magnetic resonance imaging (MRI) in St. Petersburg
MRI of the brain. T1-weighted MRI with contrast. Multiple meningiomas in neurofibromatosis type 2. Color processing of the image.
Phakomatoses (neurocutaneous disorders) are a group of congenital dysplasias of the embryonic ectoderm (skin, central and peripheral nervous systems, eyes) and endoderm (epithelial lining of the gastrointestinal tract).
Phakomatoses include:
- Neurofibromatosis type I (Recklinghausen disease)
- Neurofibromatosis type II
- Tuberous sclerosis (Bourneville syndrome)
- Hippel-Lindau disease
- Sturge-Weber syndrome
- Rare diseases – Klippel-Trenaunay-Weber syndrome, Proteus syndrome, Osler-Rendu-Weber syndrome, Wyburn-Mason syndrome, Fabry disease, cutaneous hemangioma syndrome, ataxia-telangiectasia (Louis-Bar syndrome), meningoangiomatosis (Ullmann syndrome), neurocutaneous melanosis , Ito hypomelanosis, epidermal nevus syndrome, basal cell nevus.
All of these diseases are detected by MRI of the brain.
Neurofibromatosis type I (Recklinghausen disease) has an autosomal dominant type of inheritance (50%), linked to the 17th pair of chromosomes, or its spontaneous mutations. The incidence of the disease is one in 4000 population. Diagnostic criteria are (National Institutes of Health, 1988) at least 6 skin spots (café-au-lait macules measuring at least 5 mm in the pre- and 15 mm in the postpubertal period), and at least 2 of any neurofibromas, or one plexiform (subcutaneous) neurofibroma, multiple freckles in the axillary and inguinal areas, bone dysplasias (thinning of the cortical substance of the long bones with or without coxarthrosis, sphenoid dysplasia), bilateral optic nerve gliomas, 2 or more pigmented iris hamartomas (Lisch nodes) and having a close relative with this disease. To make a diagnosis, the presence of 2 of the listed criteria is sufficient. In addition, the following concomitant pathologies are characteristic: neuromas, cutaneous neurofibromas, macrocephaly, astrocytomas, multiple meningiomas, kyphoscoliosis, Ewing's sarcoma, syringomyelia. Of the brain tumors, the most common (in 5-15% of cases of NF I) is pilocytic astrocytoma of the optic nerve and tract. On MRI, astrocytoma is visible as thickening of the optic nerve. The mass is isointense or slightly hypointense on T1-weighted MRI and hyperintense on T2-weighted MRI . Among other localizations, astrocytoma may be in the brainstem, hypothalamus, or third ventricle. Anaplastic astrocytomas of the hemispheres and cerebellum are rarely found. In children with NF I, there are lesions resembling hamartomas. They are detected in the cerebral peduncles, pons, globus pallidus, midbrain, thalamus optic, medulla oblongata, and less commonly in the white matter of the hemispheres and cerebellum. On T2-weighted MRI, the lesions are slightly hyperintense; on T1-weighted MRI, they are isointense to the white matter, with the exception of the globus pallidus, where they are also slightly hyperintense. They do not exceed 15 mm in size, do not cause mass effect and do not contrast. Presumably, the lesions are areas of altered myelin.
The third formation diagnosed in neurofibromatosis type I is a neurofibroma, usually located in the orbit and extending into the cranial cavity and cavernous sinus. Neurofibroma is slightly hyperintense to muscle on T1-weighted MRI and markedly hyperintense on T2-weighted MRI . The cystic component of the tumor may show reduced signal at its center on T1-weighted tomograms. In neurofibromatosis type I, ectasia of the dura mater in the dilated auditory canal and stenosis of the aqueduct also occur. It is important not to confuse ectasia with neuroma. Aqueductal stenosis is not associated with tumor compression, but leads to hydrocephalus.
Neurofibromatosis type II also has an autosomal dominant mode of inheritance, but linked to the 22nd pair of chromosomes. Its frequency is one per 100 thousand population. Diagnostic criteria are (National Institutes of Health, 1988) bilateral acoustic neuromas detected on CT or MRI , or a combination of hereditary predisposition (presence of bilateral neuromas in a close relative) with a unilateral neuroma or two other typical tumors (plexiform neurofibroma, meningioma, glioma, neuroma of any location) plus skin spots. Unlike NF I, skin spots are single and do not serve as the main criterion, and tumor lesions are associated not with astrocytomas, but with neuromas and meningioma. Associated pathologies are meningoangiomatosis, glial nodes, ependymal ectopia, hypertrophic gliosis of the optic nerve, syringomyelia, Arnold-Chiari complex. A typical neuroma develops from the Schwann membrane of the auditory nerves (VIII pair), usually on both sides, rarely the trigeminal nerve or others. On MRI, neuromas are hypo- or isointense to white matter on T1-weighted MRIs and iso- or hyperintense on T2-weighted MRIs . Well enhanced by gadolinium. Meningiomas usually accompany neuromas. The location does not differ from cases not associated with neurofibromatosis, but atypical lesions of the choroid plexus also occur. The picture of meningiomas in neurofibromatosis type II has all the typical features.
Tuberous sclerosis (Bourneville syndrome) is less common than neurofibromatosis. Its frequency according to the literature is about one per 180 thousand population. From 20 to 40% of cases of tuberous sclerosis are inherited in an autosomal dominant manner, the rest arose due to mutations of presumably 9 and 11 pairs of chromosomes (type 1), or 19 pairs (type 2). The lesion can affect almost any organ. Pathognomonic lesions of the central nervous system are cortical nodes in the brain and multiple subependymal glial nodes, as well as intraventricular giant cell astrocytoma; there are associated anomalies - agenesis of the corpus callosum, pachygyria, aneurysms. Characteristic dermatological manifestations are multiple facial angiofibromas in the shape of a “butterfly”, pale spots on the face and chest, fibromas of the skin, under the nails and the retina. Other manifestations include multiple angiolipomas of the kidneys and liver, cardiac rhabdomyomas, pulmonary lymphangiomatosis, bone sclerotic and cystic changes. The diagnosis of tuberous sclerosis is made if the patient has 2 of the listed characteristic signs.
Cortical nodes are the most common manifestation of tuberous sclerosis. They are located in the cerebral cortex, deform it, capture the adjacent white matter and undergo calcification. On MRI, the nodules are isointense to gray matter on T1-weighted MRIs and slightly hyperintense to gray matter on T2-weighted MRIs. Contrasting is observed in 5% of cases. The white matter contains cords extending radially from the ventricles. Cortical nodules and cords are often called “hamartomas,” although they represent demyelination and calcification rather than true heterotopia.
Tuberous sclerosis. Hamartomas. CT, T2-dependent MRI and FLAIR
Intraventricular giant cell astrocytoma occurs in 1.7–18% of patients. Its frequency peaks between the ages of 8 and 16 years. The tumor is benign and grows slowly. It is located subependymal in the area of the foramina of Monroe, causing an obstructive type of hydrocephalus. On MRI, giant cell astrocytoma is well-circumscribed, hyperintense on T2-weighted MRI , and hypointense on T1-weighted MRI . The internal structure may be heterogeneous due to hemorrhages and calcifications. The tumor is well contrasted with gadolinium. Although giant cell astrocytoma is the most common, any other neuroepithelial tumor, hemangioma, or angioma can occur in tuberous sclerosis.
Subependymal, that is, projecting into the ventricle, but growing from the side of the brain parenchyma, nodes are most often located next to the caudate nucleus or the hypothalamic sulcus immediately behind the foramen of Monro, less often in the region of the III, IV ventricles and the Sylvian aqueduct. On T2-weighted CT scans, subependymal nodes are moderately hyperintense and often contain calcifications. They are distinguished from astrocytomas by a less bright signal and smaller size. Contrasting with the administration of gadolinium drugs is sometimes observed in subependymal nodes, and always in astrocytomas.
Tuberous sclerosis. Subependymal nodes. Axial T-dependent MRI.
Hippel-Lindau disease is a symptom complex consisting of hemangioblastomas of the central nervous system (40% of cases) and retina (45%), and visceral manifestations in the form of cysts of the kidneys (75%), liver and pancreas. The diagnosis is made in the presence of two or more hemangioblastomas or one hemangioblastoma and visceral changes, or only visceral manifestations in the presence of family heredity. Hippel-Lindau disease in 20% of cases has a congenital family origin with an autosomal dominant type of inheritance, in the rest it is associated with a mutation of the 3rd pair of chromosomes. The frequency is approximately 1 case per 36 thousand population. In addition to hemangioblastomas and characteristic visceral changes in Hippel-Lindau disease, there are concomitant pathologies: kidney carcinoma (more than a quarter of cases) and pancreas, pheochromocytoma (about 10%, often bilateral), cardiac rhabdomyoma, lung cysts, epididymitis.
Hemangioblastomas in Hippel-Lindau disease are always multiple and in approximately half of the cases are localized in the cerebellum, less often in the brainstem, spinal cord and hemispheres. With cerebellar localization, the tumor is often located superficially. MRI reveals a heterogeneous nodule, hyperintense on T2-weighted and iso- or hypointense on T1- weighted MRI . In some cases, pathologically dilated vessels are visualized, with a characteristic lack of signal. No calcification of the nodes is observed. Hemangioblastomas are well contrasted with gadolinium. Pure solid hemangioblastomas are observed in only 10% of cases. The cyst surrounding the node is hyperintense on tomograms of both types of suspension, as it contains an admixture of protein.
Sturge-Weber syndrome is a non-inherited disease; its morphological substrate is angiomatosis, associated with the fact that sinusoidal embryonic vessels are preserved. Thus, Sturge-Weber syndrome is a developmental anomaly in its “pure” form. Arterial and venous angiomatosis lead to excessive vascularization of the meninges and calcification of the meningeal arteries. The soft meninges are affected, usually the occipital lobe, and on one side (75% of cases). The cerebral cortex above the angioma atrophies and calcifies. A pathologically dilated cortical vein is often detected. Enlargement of the choroid plexus, hemiatrophy of the brain on the affected side, acceleration and disruption of myelination, megalencephaly and hydrocephalus have also been described. The presence of a forehead skin nevus, which is located along the first branch of the trigeminal nerve, on the same side as the lesion in the brain, helps in making the diagnosis. Other manifestations of the disease include bone - ipsilateral hypertrophy of the skull and sinuses, ocular - ipsilateral exophthalmos, glaucoma (30%), coloboma of the iris, hemangioma of the choroid plexus of the eye, visceral - angiomatosis of the thyroid gland, lungs, pancreas, liver, kidneys, intestines. Clinically, the syndrome manifests itself as contralateral hemiparesis, homonymous hemianopia, seizures (80% of cases) and mental retardation (60%). MRI reveals a well-enhanced angiomatous tangle of vessels, a thickened membrane, a dilated cortical vein and, sometimes, a dilated choroid plexus .
MRI of St. Petersburg provides the place of choice for performing MRI of the brain. With MRI in St. Petersburg, we advocate an integrated approach to the diagnosis of phakomatoses with the study of all their manifestations. Typically, phakomatoses are better visible in high fields, but many, especially tumors, are also visible in low-field open MRIs.
Leave feedback.
MRI in St. Petersburg USA
Clinic of phakomatosis
Polymorphic damage to the skin, nervous system, and internal organs is a characteristic sign of phakomatosis. Signs of neurological and dermatological syndromes appear in early childhood, as they are congenital. Much later other signs appear. In some clinical cases, phakomatosis occurs against the background of congenital immunodeficiency, combined with premature aging and the risk of developing cancer.
Lesions of the nervous system are expressed in formations in the medulla and membranes. Most often, cysts, subependymal nodes, neurofibromas, calcifications, and areas of atrophy or demyelination appear. The patient is diagnosed with congenital anomalies of the cerebral vessels - aneurysms, angiomas. Often a convulsive syndrome appears with various forms of attacks.
West syndrome is recorded in early childhood. Older children experience generalized and partial sensorimotor epileptic seizures, and Lennox-Gastaut syndrome manifests itself. Epileptic seizures and disorders of brain structures lead to mental retardation, speech disorders, mental retardation, and abnormal behavior. The degree of mental retardation is related to the frequency and severity of epileptic seizures and can vary from debility to idiocy.
Patients experience disorders in the functioning of the cranial nerves - oculomotor disorders, hearing pathologies, paresis of the facial nerve. There are signs of cerebellar ataxia, sleep disorganization in the form of insomnia or somnambulism. From the extrapyramidal areas - tonic muscle symptoms, hyperkinesia, bradykinesia. The patient's behavior is disrupted until the development of ADHD or autism.
Metamorphoses of the skin with phakomatoses appear in the first months of life. The spots on the skin are asymmetrical, can have different colors, sizes, single or multiple. Patients most often experience age spots, dermatofibromas, areas of reduced pigmentation, papillomas, angiomas, and shagreen plaques.
The phenomena of phakomatosis are accompanied by disorders of the endocrine system in the form of diabetes insipidus, hypothyroidism, and obesity. Children experience delayed or early puberty, and on the part of the autonomic nervous system - trophic disorders in the form of brittle nails, dry skin, and hair loss. Ophthalmologists detect damage to the visual organs of congenital origin or early manifestation. During the examination, angiomatosis, retinal hamartomas, and conjunctival telangiectasia are detected. There is a decrease in the quality of vision.
On the part of the internal organs, the development of neoplasms is noted. Most often, tumors are benign in origin, but they can recur and progress. Children suffering from phakomatosis are more prone to infectious diseases than others, which lead to complications from the underlying disease.
Classification of diseases
The term “phakomatosis” cannot be used as a diagnosis; it denotes the relationship of the pathology to a certain group of neurocutaneous diseases; there is a classification, based on which the most common forms among them are:
- Recklinghausen's disease (neurofibromatosis type 1) is an incurable progressive pathology with a large number of nodular growths (neurofibromas), pigment spots on the coffee-colored skin, tumors of the nervous system and abnormalities of the musculoskeletal system;
- neurofibromatosis type 2 - characterized by multiple, more active tumors, in particular bilateral symmetrical acoustic neuroma;
Tuberous sclerosis - Bourneville's disease (tuberous sclerosis) - characterized by benign tumors in many organs, epileptic seizures, adenomas of the sebaceous glands, mental retardation in children;
- Sturge or Sturge-Weber syndrome (encephalotrigeminal hemangioblastosis) - congenital cherry nevus on the face, vascular tumors of the retina and brain, secondary glaucoma;
- Klippel-Trinone syndrome (hypertrophic hemangioectasia) - flaming nevus in the extremities, varicose veins, partial gigantism of the affected part of the body due to the proliferation of arteriovenous anastomoses and excessive vascularization;
- Louis-Bar syndrome - a combination of cerebral ataxia and telangiectasia, congenital immunodeficiency;
- Rendu-Osler disease - telangiectasia of the skin and mucous membranes, vascular pathology in the internal organs, bleeding and chronic anemia;
- Hippel-Lindau syndrome - multiple hemangiomas in the brain and spinal cord, retina, internal organs;
- Bonnet-Deschoma-Blanc disease (neuroretinal hemangiomatosis) - excessive proliferation of blood vessels and damage to the retina, but without secondary glaucoma;
- Bloch-Sulzberg melanoblastosis - in females, hyperpigmentation and inflammation of the skin in combination with damage to the nervous system, abnormalities of the eyes, skeleton and internal organs (the male fetus dies);
- Ito hypomelanosis - skin pigment spots in combination with epileptic seizures, musculoskeletal and cerebral abnormalities.
Diagnosis of the disease
The variety of clinical symptoms and their manifestations at different ages make it somewhat difficult to make a correct diagnosis. For a correct conclusion, you should consult a neurologist, pediatrician, ophthalmologist, dermatologist, cardiologist, nephrologist, geneticist, endocrinologist. A biochemical examination of blood and urine, genetic analysis, DNA examination, and examination of the neuropsychological state are prescribed.
Hardware methods include:
- electroencephalography - reveals the nature of epileptic activity of the brain;
- Echo-EG - detects hydrocephalus;
- MRI, CT - provide information about changes in brain tissue;
- cerebral angiography - abnormalities in the development of cerebral vessels;
- ophthalmoscopy - reveals vision pathologies, even without an obvious clinical picture;
- ECG, ultrasound of the heart - to determine cardiac changes.
If other types of pathology are suspected, ultrasound of the abdominal cavity, radiography of the stomach, examination of the intestines using a contrast agent, ultrasound of the kidneys, and urography are prescribed.
Treatment of phakomatosis
Specific therapy for phakomatoses has not been developed. Treatment is aimed at eliminating symptoms. In accordance with the clinical manifestations, anticonvulsants, dehydrating, and neurometabolic drugs are prescribed. Epileptic seizures can be very resistant to anticonvulsants, which requires a change in drug or a combination of two drugs. Stimulating neurometabolites are not prescribed in the presence of epileptic episodes, as they have an exciting effect.
Surgical intervention is performed in the presence of malignant neoplasms. The operation is performed when the tumor is actively growing and there are signs of compression. Neurosurgical operations are performed when intracerebral formations are detected.
Patients are required to undergo psychocorrection aimed at stimulating the child’s mental and mental qualities, his learning and social adaptation. It is advisable to conduct classes with a child psychologist, play therapy, and neuropsychological correction. Psychological counseling of parents is mandatory.
Therapeutic measures
Specific treatment methods have not been determined at the present stage. In accordance with the symptomatic picture, anticonvulsant, dehydrating, and neurometabolic drugs are prescribed.
Often epileptic seizures turn out to be tolerant to the ongoing anticonvulsant therapy, so they come to combined treatment, which is based on at least two anticonvulsants.
In case of episyndrome, it is strictly forbidden to use stimulating neurometabolites (GABA, piracetam, pyritinol).
In accordance with the indications, surgical treatment is prescribed to remove the malignant neoplasm, especially if it is located intracranial.
An important role is played by psychocorrection, which is aimed at developing the mental and psychological capabilities of the child, individual correction of deviations, teaching children in an accessible form and their social adaptation.
Forecast and prevention of phakomatosis
Phakomatoses in most clinical cases are diseases that have an unfavorable prognosis. The form of the disease, the age of the child at which the diagnosis was first made, and the severity of clinical symptoms have an impact on the final outcome of the disease. An infectious disease or injury can complicate the course of the disease.
Early manifestation of phakomatosis, severe course of epileptic seizures, severe mental retardation, the appearance of malignant tumors - all this significantly aggravates the prognosis of the disease. The patient may die from cerebral edema during an epileptic attack, cachexia in severe cancer, or sepsis.
Preventing the birth of a sick child is the main way to prevent the development of phakomatosis. Parents planning to have a child should undergo genetic counseling.
Clinical manifestations
All phakomatoses are characterized by pronounced polymorphism of skin manifestations, damage to various structures of the nervous system and visceral organs.
It is characteristic that at an early age, mainly dermatological symptoms are detected, and neurological and others are detected later. In some cases, phakomatosis is combined with congenital deficiency of the immune system (Louis-Bart disease), premature development of aging and (or) the risk of tumor malignancy.
Damage to the central nervous system in this pathology morphologically looks like a proliferation in the membranes and brain tissue of nodules, cystic cavities, neurofibromatous formations, areas of demyelination, atrophy and calcification, congenital vascular anomalies such as aneurysms, hemangiomas.
In the clinic there is a picture of convulsive syndrome with a different nature of the course. Children often experience epileptic seizures, as a result of which phakomatosis is often accompanied by delayed neuropsychic development, mental retardation, and antisocial behavior. The severity of mental retardation is directly proportional to the severity and frequency of epileptic seizures.
The group of diseases is characterized by lesions of different pairs of cranial nerves with the development of oculomotor, auditory disorders, paresis and other symptoms.
There may be pyramidal insufficiency (often unilateral), extrapyramidal disorders (brady and oligokinesia, hyperkinesia, tonic muscle spasms), cerebellar dysfunction (coordination problems), and sleep function disorders.
Dermatological manifestations are usually detected in the first weeks or months of life. Elements of the rash can be single or widespread, of different colors and sizes, often asymmetrical.
Pigment spots of different shades of brown, areas of reduced pigmentation, nodular elements, neurofibromas, papillomas, shagreen skin with plaques, hemangiomas are considered typical.
In some cases, phakomatosis occurs with endocrine disorders such as obesity, diabetes insipidus, and disorders of normal sexual development. There are symptoms of a vegetative-trophic nature (hair loss, brittle nails, dryness and flaking of the skin).
Quite often there is eye damage, which manifests itself quite early after the birth of the child. Upon examination, retinal hemangiomatosis and persistent pathological dilatation of conjunctival vessels are revealed. It may be asymptomatic and manifest only in the form of reduced visual acuity.
Lesions of internal organs are structurally and functionally caused by tumors developing in them, which often have a benign growth pattern, but are prone to frequent recurrence and progression.
In addition, reduced immunity in children with phakomatosis contributes to the tendency to acquire various infections that worsen the course of the underlying disease.