Heat
The patient's temperature rises sharply - up to 40°C - and fever begins. This is one of the first signs of meningitis. An unfavorable symptom is body temperature below normal. There is also a localized form of meningitis, when the infected person himself is not sick, but is a carrier of the infection, or the disease is mild, resembling ARVI. Then the temperature reaches 38°C. Doctors recommend going to the hospital even if you suspect localized meningitis, as the disease can become severe.
Photo: spinoff.com
Classification
It's time to look directly at the symptoms themselves, which are commonly called meningeal. The meningeal symptom complex includes:
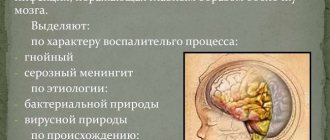
a — pointing dog pose, b — Kernig’s sign, c — Brudzinski’s sign
- Kernig's sign
- Brudzinski syndrome
- headache
- vomit
- Bekhterev's symptom
- Gordon's reflex
- Guillain's reflex
- Le Sage syndrome
- stiff neck muscles
- presence of a “pointing dog” pose
- hyperesthesia
Kernig's sign
To diagnose a syndrome such as Kernig's symptom, the patient is asked to take a supine position, after which the doctor bends his leg at the hip and knee joints at an angle of 90°. Flexion occurs unhindered, but problems arise with extension. So, due to tension in the muscles of the back of the thigh, the patient cannot do this on his own.
Brudzinski syndrome
Brudzinski meningeal syndrome has several variations, including:
- Buccal.
- Lower.
- Upper.
- Average.
Buccal – the doctor applies pressure to the patient’s cheek, resulting in involuntary flexion of the arms at the elbow joint, as well as a kind of shrug of the shoulders.
Lower - With the patient sitting, one of the legs is bent, the second automatically bends along with the first.
Upper – the patient’s head is tilted forward, and the legs are automatically bent.
Medium – when pressing on the patient’s pubis, the legs bend.
Often, Kernig and Brudzinski syndromes occur together in meningitis.
Headache
When meningitis occurs, headache accompanies the patient constantly and does not stop for a minute. It is one of the most pronounced meningeal symptoms.
Vomit
Gag reflexes can occur in a patient even in the absence of such manifestations as primary symptoms, such as nausea. Vomiting occurs suddenly against the background of a severe headache and is characterized by a gushing outpouring.
In some cases, there is a decrease in the intensity of headaches after bouts of vomiting.
Bechterew's syndrome
Meningeal ankylosing spondylitis is diagnosed by tapping the patient's cheekbone with a finger. This tapping causes a severe headache on the side of the face where there is inflammation, in addition, this side will curl up in a grimace of pain.
Gordon reflex
Gordon's meningeal syndrome is diagnosed by a neurologist as follows: the doctor wraps his hand around the patient's lower leg and applies strong compression. As a result, the patient's big toe unclenches, and the fingers also diverge in different directions.
Guillain reflex
The patient is asked to take a lying position, after which the doctor applies pressure on the front surface of the thigh of one of the legs or squeezes it. As a result, the opposite leg involuntarily bends at the knee.
Lesage syndrome
This symptom is typical for infants, and in most cases it is diagnosed in them. The patient lifts himself by the armpits above the floor, as a result of which the baby's legs involuntarily tighten (are pulled towards the chest).
Neck muscle stiffness
This condition is characterized by hypertonicity of the occipital and cervical muscles and manifests itself in the inability or difficulty in performing simple actions, such as turning the head or tilting it.
Often, muscle rigidity is characteristic of young children, but not as a symptom of meningitis, but due to the fact that the peripheral nervous system is not fully formed. Therefore, it is extremely important to diagnose the disease comprehensively and be based on several factors.
Pointing dog pose
In some sources there is such a name as the “cocked hammer” pose. It manifests itself as follows: the patient throws his head back, the torso is tense and elongated, the arms are pressed tightly to the chest, the legs are also pulled up to the thoracic region.
Hyperesthesia
Meningeal hyperesthesia syndrome, or increased light and noise sensitivity, manifests itself in the form of painful perception by the patient of bright light and loud sounds. For this reason, the patient is recommended to stay in a darkened room and, if possible, completely eliminate irritating sounds.
Diagnosis of the syndrome
To determine meningitis, specialists resort to the following diagnostic methods:
- Anamnesis.
The patient is diagnosed with chronic diseases and infectious pathologies suffered in the recent past. - Visual
inspection. It includes a consultation with a neurologist, analysis of the somatic condition (pulse, skin condition, blood pressure), examination of the mucous membranes of the nasopharynx and oral cavity. - Laboratory analysis.
The most important test to detect meningitis is a lumbar puncture to further analyze the cerebrospinal fluid. - Instrumental
tests - MRI or CT, skull x-ray, echoencephaloscopy.
With purulent meningeal syndrome, turbidity of the CSF is noted. The analysis shows a high content of neutrophils in the substance and an overestimated number of cells. In the serous type of the disease, the CSF is transparent and consists predominantly of lymphocytes.
Cytosis in this case is 200-300 cells per 1 μl. To make the examination results more reliable, the procedure is repeated 8-12 hours after the lumbar puncture.
Treatment
If there is a suspicion of a disease, help should be urgent. To prevent complications such as epilepsy, dementia, hearing loss and other negative phenomena, therapy is carried out in an inpatient setting. The patient is prescribed bed rest, and a drip is used to relieve intoxication. Treatment is carried out with drugs:
- Antibacterial action: “Mernem”, “Ceftriaxone”, “Chloramphenicol”.
- Against viral nature: “DNA-ase”, “Interferon”, “RNA-ase” and lytic mixture.
- Painkillers and antipyretics: “Acetylene”, “Paracetamol”, “Panadol”.
- Sedatives: “Seduxen”, “Dikam”, Diazepam.”
- Corticosteroid hormones: Novomethasone, Dexamethasone, Methylprednisolone.
- Antifungal: Diflucan, Fungolon, Flucostat.
Therapy is carried out with an individual dosage and course of treatment under the supervision of a doctor.
Concept of meningeal syndrome
The concept of the syndrome includes the following symptoms:
- cerebral;
- general infectious;
- meningeal.
Along with the listed signs, there is a disturbance in the dynamics of the liquor fluid and pathological changes in the spinal substance.
General cerebral symptoms are the reaction of the central nervous system to inflammatory processes occurring in the membranes of the brain. With any type of meningitis, signs characteristic of infectious diseases are observed.
Meningeal symptoms are manifested by an increased reaction of the sensory organs to external factors, changes in reflex functions and muscle tension.
Video about meningeal symptoms
– a symptom complex characteristic of damage to the cerebral membranes. It may have an infectious, toxic, liquor-hypertensive, vascular, traumatic, carcinomatous etiology. Manifested by headache, muscle rigidity, vomiting, hyperesthesia, algic phenomena. The diagnostic basis is made up of clinical data and the results of cerebrospinal fluid examination. Treatment is carried out according to the etiology with antibacterial, antiviral, antifungal, antiprotozoal agents, including symptomatic therapy, reducing intracranial pressure.
Existing diagnostic tests
Determining the disease is not difficult: you need to check whether the patient has characteristic symptoms. It is necessary to carry out monitoring, referring to meningeal signs. The procedure is shown in the photo.
The analysis is carried out according to the following criteria:
- Tilt of the head forward meets resistance from the back of the head (muscle rigidity).
- When lying on your back, the leg bent at the knee resists straightening (Kernig's syndrome).
- When the lower limb is flexed, the second limb is simultaneously affected (according to Brudzinsky).
The main meningeal symptoms are a reason for further investigation. Diagnostic activities include:
- lumbar puncture of the spinal cord and brain;
- cerebrospinal fluid cytology;
- computed tomography;
- blood test to detect antibodies (immunological);
- scraping from the mucous membrane for diplococcus.
If necessary, hypsarrhythmia is performed using an EEG (electroencephalogram).
Prognosis and prevention
In most cases, timely and correct treatment leads to the patient’s recovery. Residual effects may be observed for several months: asthenia, emotional lability, cephalgia, intracranial hypertension. An unfavorable outcome is meningeal syndrome, which accompanies a severe disease of the central nervous system, a fulminant course of the infectious process, and oncopathology. Prevention of meningeal syndrome includes increasing immunity, preventing infectious diseases, injuries, intoxications, and timely treatment of cerebrovascular and cardiovascular pathologies. Specific prevention is possible against meningococcal and pneumococcal infections.
Meningeal syndrome is a set of symptoms of such a dangerous disease as meningitis, accompanied by inflammation of the meninges. The treatment regimen for the pathology depends on the form of its manifestation and the causes of its occurrence. The syndrome occurs with any type of meningitis.
Etiology of the disease
The pathology may be based on various pathogens that begin to develop against the background of a weakened immune system. Responsible for bacterial meningitis in children:
- pneumo- and meningococci;
- streptococci and staphylococci;
- hemophilus influenzae;
- tuberculosis;
- enterobacteria;
- spirochetes;
- rickettsia.
The aseptic type of disease is caused by viruses:
- enterovirus infection;
- microorganism Coxsackie;
- mumps, or so-called mumps;
- polio;
- encephalitis tick bite;
- chicken pox;
- rubella;
- measles;
- adeno- and ECHO viruses;
- herpes.
Symptoms appear a few hours after the attack, in rare cases - within a day. And also childhood meningitis can be caused by pathogenic fungi, malarial plasmodium or various types of helminths.
The infection is transmitted directly through mucus fragments when sneezing or coughing. Pathological pathogens enter the body through the nasopharynx. The disease has an incubation period, when symptoms have not yet appeared and the person is contagious. A number of pathologies can also cause meningitis:
- inflammatory infections in the respiratory system;
- otitis, adenoiditis;
- abnormal structure of the skull, deviated nasal septum, sinusitis;
- furunculosis localized on the front part, caries;
- avitaminosis.
The development of pathology in infants is provoked by:
- intrauterine infections;
- fetal prematurity;
- hypoxia during complicated childbirth.
At an early age, poor care, hypothermia, climate change and excessive physical activity contribute to the disease. The anomaly occurs against the background of an unformed immune system and weak resistance of the blood-brain barrier.