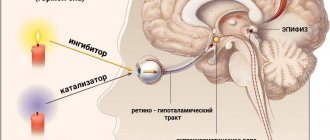
What is the pineal gland and what is it for?
The pineal gland is located in the brain, near the third ventricle, and produces a number of hormones (for example, melatonin, an essential sleep hormone).
A pineal gland tumor occurs in 1-1.5% of all GM tumors and has many subtypes presented below.
Frequency:
- Pineoblastoma 145% of all pineal tumors
- Germinoma – 0.3% of all brain tumors
- Pineocytoma - 1% of all brain tumors.
Gender distribution:
- Pineoblastoma - more common in men
- Germinoma - M:F 12:1
- Pineocytoma - males and females are affected equally often.
Peak age:
- Pineoblastoma – 0-20 years
- Germinoma - 10-20 years
- Pineocytoma - 20-40 years.
Reasons for appearance
- Tumors arising from the pineal gland
- Benign tumors (pineal cyst, pineocytoma, teratoma, dermoid) are differentiated from malignant tumors (germinoma, pineoblastoma, choriocarcinoma)
- Tumors arising from pinealocytes are divided into grades depending on their malignancy
- Germinomas develop from primitive germ cells; Teratomas typically consist of ectodermal, endodermal and mesenchymal components of varying degrees of differentiation (mature teratoma, teratocarcinoma).
Symptoms of the disease
The earliest sign of pineocytoma is headache. It is the result of high intracranial pressure due to compression of the cerebrospinal fluid outflow tract. Occurs in the form of attacks with:
- dizziness;
- nausea and vomiting that does not bring relief;
- ringing, noise in the ears;
- forced position of the head (freeze in a half-tilt forward);
- pressure on the eyes, feeling of fullness;
- numbness of the face and body parts;
- nosebleeds;
- darkening of the eyes.
As the tumor grows, the pain becomes almost constant and is not relieved by conventional painkillers. Then visual impairment occurs. It is associated with the pressure of the tumor on the nearby optic chiasm.
Depending on the direction of growth
All other symptoms depend on which direction the pinealoma will grow:
- cerebellum - unsteadiness when walking, difficulty coordinating movements, sweeping handwriting, muscle weakness, hand tremors; as the patient progresses, the patient cannot stand or sit steadily;
- up, towards the quadrigeminal tubercles - inability to look up, convergent squint or one eye looks up and out, and the other in and down, drooping eyelids, double vision, absence or uneven reaction of the pupil to light;
- hypothalamus – loss of appetite or its sharp increase, increased body temperature, thirst and frequent urination, dehydration (diabetes insipidus), obesity, constant drowsiness;
- pituitary gland - disturbances in vision, thyroid function, growth, adrenal function, reproductive function.
Watch the video about the symptoms of pinealoma:
At a late stage
At a late stage, a large tumor disrupts the conduction of impulses from the brain. This manifests itself in episodes of sharp deterioration of the condition – crises:
- increased tone of the muscles that extend the limbs and neck;
- twitching of the pupils of the eyes, reminiscent of tracking a moving object (nystagmus);
- loss of consciousness;
- changes in pressure and pulse rate.
With a malignant tumor, symptoms increase rapidly. Characterized by the appearance of foci of metastases in the spinal cord, which cause various disturbances of movement and sensitivity.
MRI of pineal tumor
Pineoblastoma has a developed network of blood vessels. They are thin, so if they rupture, hemorrhage is possible, including life-threatening intraventricular hemorrhage.
Effect on the body
The pineal gland, when a tumor develops in it, loses control over the functioning of the gonads and the nervous system. As a result, violations arise:
- early maturation of children - milk teeth change prematurely, growth is ahead of peers;
- sexual characteristics appear prematurely;
- in boys, the scrotum and penis increase in size, hair begins to grow on the face and in the armpits, in the groin area;
- in girls, mammary glands form, menstruation begins prematurely, sexual excitability increases, and uterine bleeding is possible.
Such changes may not always occur. If, as a result of tumor growth, it stimulates the functions of the pineal gland, that is, it has independent hormonal activity, then the level of melatonin increases.
It suppresses the functioning of the gonads, which is manifested by delayed physical and sexual development. One of the characteristic signs is sleep disturbance. It occurs in the form of insomnia, drowsiness, and jet lag—sleeping during the day and staying awake at night.
Character of neoplasms
There are benign, cancerous and mixed tumors. The first are formed from pineal gland cells - pineocytes. Their structure and functions are very similar to the rods and cones of the eye, which detect light. When specificity (signs of functioning tissue) is lost, the neoplasm becomes cancerous.
There are 3 types of tumor processes in the pineal gland tissue:
- benign differentiated;
- mixed or intermediate structure (there are typical and atypical pineocytes);
- malignant undifferentiated - cells completely lose their structure, quickly begin to divide and spread to neighboring areas of the brain.
Approximately 35% of all pineal tumors are cancerous. This is a fairly high figure; at least 42% are mixed, that is, prone to malignancy. Therefore, until the exact structure is confirmed, all detected pineal gland neoplasms are considered potentially malignant.
Not only pinealomas are found in the pineal gland itself. The tumor may come from:
- germ cells that have not moved to their normal location - the ovaries and testes (germinoma, teratoma), they are similar in structure to neoplasms of the gonads;
- glial cell elements (auxiliary fibers of nervous tissue) - gliomas make up at least 25% of all tumors of the pineal gland, grow quickly, but do not have a tendency to move to other tissues (do not metastasize).
Diagnostic methods
Tumors of the pineal gland are dangerous because their symptoms may be absent for a very long time, and when the patient goes to the doctor with constant headaches and attacks of loss of consciousness, this is already an advanced stage of the disease.
Help to make a correct diagnosis:
- examination by a neurologist - changes in muscle tone and reflexes, signs of pathology of the oculomotor nerves, instability when performing coordination tests, eating and drinking disorders (hypothalamic syndrome);
- examination by an ophthalmologist - congestion in the fundus, swelling of the optic discs, blurred vision;
- echoencephalography – signal displacement in deep zones;
- electromyography and electroneurography to assess the function of muscles and nerve fibers, which is important when movement and sensitivity are impaired;
- spinal cord puncture - increased protein levels in the cerebrospinal fluid, increased cells, alpha-fetoprotein content, beta-chorionic gonadotropin (tumor markers).
Based on these data, a tumor in the brain can be suspected, and to identify its location, the following is carried out:
- MRI - layer-by-layer scanning gives dimensions, exact location, stage, direction of growth, germination into neighboring tissues;
- CT or multislice CT – performed if it is impossible to undergo an MRI (contraindications);
- angiography – necessary to assess the condition of blood vessels, it is prescribed with MRI or CT control;
- ventriculography – the ventricles of the brain are filled with contrast to exclude tumor growth in them, which is important for deciding on surgery.
MRI of the brain
Modern treatment
The most preferred treatment for pinealoma is surgery. It goes through craniotomy. Due to the location of the pineal gland in the deep part of the brain, near vital centers, it is considered extremely dangerous. Mortality rates after the procedure are close to 65%. Therefore, neurosurgeons rarely resort to surgical removal. If it is nevertheless prescribed, then the tissue must be taken for analysis and if cancer cells are detected, the operation is supplemented with radiation.
An alternative option is stereotactic destruction of the pinealoma. The essence of this modern treatment method is to direct radioactive rays at the tumor from different directions. Each of them is low-energy, that is, it does not damage brain tissue when passing through. They meet at a pre-calculated point - the center of the neoplasm. This leads to the death of tumor cells while preserving healthy ones.
Gamma knife treatment
They use Gamma Knife, Novalis and Cyber Knife. An important feature of the latter method is the ability to control removal using tomography. Advantages of radiosurgery:
- no opening of the skull is required;
- there is no need for preparation;
- there are no postoperative complications, you can immediately begin normal activities;
- no need to administer general anesthesia, painless removal;
- high efficiency and low risk of relapse;
- used to treat patients of any age and with concomitant diseases.
The disadvantage of this method is the gradual onset of the effect. Not all pinealomas are equally sensitive to radiation. Therefore, treatment may require from 5 to 30 sessions, they are carried out every other day or 5 times a week. Schemes and the number of courses are determined by control tomograms.
Stereotactic destruction of pinealoma
If it is discovered that the tumor has spread beyond the epiphysis, then stereotactic removal can be combined with radiation. When the pinealoma is very large, you first need to try to shrink it with chemotherapy or radiation therapy sessions, and then destroy it.
In inoperable cases, shunting is used to reduce headaches and attacks of loss of consciousness. It consists of creating a pathway for the outflow of cerebrospinal fluid. It is important to consider that in the case of a cancerous tumor, tumors can spread through these shunts.
Which method of diagnosing a pineal tumor to choose: MRI or CT
Selection method
- MRI
Is a CT scan of the brain informative for a tumor of the pineal gland?
- Homogeneous tumor in the pineal region above and posterior to the quadrigeminal plate
- Calcifications may be observed, especially in germinomas and pineocytomas.
- Even small tumors can lead to disruption of cerebrospinal fluid circulation
- In contrast to the smooth contours of pineocytoma, pineoblastoma is characterized by fuzzy and uneven boundaries
- Germinomas are hyperdense in relation to the surrounding brain parenchyma
- Pineoblastomas and pineocytomas are hypodense.
What MRI scans of the brain will show for a pineal gland tumor
Pineocytoma:
- Hypointense in relation to the brain substance on T1-WI, hyperintense on T2-WI
- Homogeneous contrast enhancement
- Usually less than 3 cm.
Pineoblastoma:
- Hypointense on T1-WI, hyperintense on T2-WI
- Heterogeneous contrast enhancement
- Often more than 3 cm in size
- Lobular.
Germinoma:
- Solid tumor
- Significant contrast enhancement
- Metastases in the liquor space.
Teratoma:
- Ring contrast enhancement
- An intratumoral cyst may be detected
- The signal varies depending on the content of the three cell types.
Choriocarcinoma:
- Hemorrhages are characteristic
- At the same time, there is contrast enhancement of the tumor and areas of necrosis, hypointense on T1-weighted images.