Author's rating
Author of the article
Shoshina Vera Nikolaevna
Therapist, education: Northern Medical University. Work experience 10 years.
Articles written
218
Puncture (lumbar) for meningitis is a mandatory procedure that is performed by inserting a special needle into the patient’s lumbar spine to diagnose and treat this disease. If inflammation of the meninges (meningitis) is suspected, a puncture is considered a key step, allowing not only to accurately diagnose the disease itself or refute its presence, but also to determine the type of pathogen in order to prescribe adequate treatment.
Every person who has been prescribed a lumbar puncture treats this manipulation with fear and apprehension, considering it painful and dangerous. But undesirable consequences will be completely absent or minimized if:
- the medical staff performing the manipulation has experience and special skills to carry it out;
- the patient who is prescribed a puncture follows all the instructions of the staff during the puncture and follows all the doctor’s recommendations after the procedure.
Given the combination of these factors, the procedure takes minimal time, is virtually painless, and has no consequences.
General information about the disease
Meningitis is a dangerous disease that can cause serious consequences. The pathology is characterized by inflammation of the lining of the brain, in which a large amount of cerebrospinal fluid (CSF) begins to form, the medulla is damaged, and blood microcirculation in the vascular bed deteriorates.
The consequences of such inflammation are neurological changes that negatively affect the life and health of the patient, as well as cerebral edema - an emergency condition requiring immediate medical attention.
Factors causing the development of meningitis are divided into aseptic and purulent subtypes. The aseptic type is characterized by the viral nature of infection: enterovirus, herpes and choriomeningitis viruses. The purulent type of infection is caused by the intervention of bacteria: meningococcal, pneumococcal, staphylococcal - or external surgical influence.
For meningitis, depending on the nature of the infection, special treatment is required. To diagnose the causative agent of the disease and determine the method of therapy, a specific study of the spinal cerebrospinal fluid is performed - a puncture for meningitis.
Excess cerebrospinal fluid (cerebrospinal fluid) is produced in the cerebral ventricles. At the bottom of these areas of the brain there are plexuses of blood vessels responsible for the production of fluid. The cerebrospinal fluid passes through the ventricles and penetrates the subarachnoid space of the brain and spinal cord. Liquor is necessary to maintain an optimal level of intracranial pressure, provide shock absorption during shock and injury, and nourish brain tissue and cells. Liquor washes the lining of the brain and therefore represents a certain container for the accumulation of viruses and bacterial microorganisms during illness.
Insertion of a special needle into the subarachnoid space - lumbar puncture - is a modern and accurate method for diagnosing the causative agent of infectious meningitis using spinal cord fluid analysis.
Preparing the child
No special preparation is required before diagnosing meningitis. Culture tests are taken in the morning, on an empty stomach. Do not take antibiotics before donating blood.
Computed tomography is not performed for diseases of the thyroid gland, bronchial asthma and cardiovascular diseases. A referral for diagnostics is given by a pediatrician after a preliminary examination. The therapist is also responsible for issuing referrals. The procedures take place in clinics and private clinics.
In public clinics, consultation and examination are often carried out free of charge ; if you use paid services, the price starts from 1000 rubles. In special paid clinics, the price of consultation and examination of children starts from 3,000 rubles.
Features of the procedure
A puncture for meningitis is carried out as follows. The manipulation is carried out on the operating table, where the patient is positioned lying on his side with his legs pulled up to his chest. The head is tilted forward. The specific position of the body ensures the expansion of the intervertebral spaces, which facilitates the insertion of the needle and reduces the patient’s pain. In some cases, the procedure is performed while sitting (if the patient is overweight).
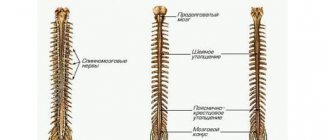
The target area from which material for analysis is taken is at the level of the 3rd – 4th lumbar vertebrae. To quickly and accurately determine the 4th vertebra, the following method is used: when connecting the iliac crests, a conditional line is drawn, which is located at the level of the desired vertebra.
The procedure is carried out under sterile conditions. The puncture site is treated with a disinfectant. After which the patient is injected with a drug for local anesthesia. The anesthetic is administered three times: intradermally, subcutaneously and additionally during manipulation.
The needle with the mandrel is inserted parallel to the spinous processes and slowly moved forward until it enters the cavity (feeling of failure). This means that the instrument has passed through the dura and ligaments and entered the subarachnoid space. An initial collection of cerebrospinal fluid is then performed to verify correct needle placement. After this, the material for research is collected into a clean test tube.
When assessing the result of the manipulation, the nature of the flow of cerebrospinal fluid into the test tube, the color and type of brain fluid are taken into account.
Normally, cerebrospinal fluid should flow out in the form of rare drops. With frequent and rapid flow, a significant increase in intracranial pressure is likely. The red tint of the secreted fluid indicates a possible hemorrhage in the subarachnoid space or damage to the vessel during puncture.
The duration of the procedure is about 7 – 10 minutes. In this case, the patient may experience quite unpleasant sensations. At the end of the manipulation, the needle is removed, the injection site is treated with an antiseptic and a bandage is applied. The patient must remain motionless for 2 to 3 hours after the puncture to eliminate the risk of cerebrospinal fluid leaking out of the hole.
A cerebrospinal fluid puncture can be taken not only to establish an accurate diagnosis and the causes of meningitis infection. The procedure is prescribed to eliminate intracranial hypertension through the direct administration of antibiotics. Also, during the manipulation, the pressure of the cerebrospinal fluid is measured and the patency of the cerebrospinal fluid tract is examined.
Characteristics of spinal canal fluid in tuberculous meningitis
Laboratory tests for microorganisms for the tuberculous type of meningitis do not show positive results. A more thorough study of the cerebrospinal fluid helps to detect the presence of a pathogen in it.
Precipitation can be noticed no earlier than 12 hours after analysis. The sediment looks like a fibrin network in the form of a web or flakes. A large number of Mycobacterium tuberculosis can be found in it.
During the tuberculous process, the cerebrospinal fluid remains transparent, without noticeable coloring. Cytosis occurs in a fairly wide range and differs depending on the stage of meningitis. In the absence of etiotropic treatment, the number of cells always increases. Repeated cerebrospinal fluid sampling after the start of therapy notes a decrease in the number of cells.
A characteristic feature of the development of pathology is the presence of lymphocytes in the cerebrospinal fluid. If the level of monocytes and macrophages in it increases, this is a bad sign. Neutrophils and giant lymphocytes can be found in large quantities in the cerebrospinal fluid. Protein in this pathology usually increases; its level can reach 3 grams per liter.
The glucose level in the cerebrospinal fluid with tuberculous meningitis sharply decreases to 0.8 mmol. Sometimes the chloride level also decreases. A favorable indicator is an increase in the level of these cerebrospinal fluid indicators.
Analysis results
Each type of meningitis is characterized by a specific type of pathogen, which will describe changes in the spinal cerebrospinal fluid.
Viral meningitis is characterized by certain changes in the cerebrospinal fluid:
- the predominance of the concentration of lymphocytes over the content of leukocytes in percentage terms;
- absence of bacterial microorganisms in the sown material;
- clear color of cerebrospinal fluid.
Bacterial meningitis is accompanied by the following changes in the cerebrospinal fluid:
- increase in the number of neutrophils (above 1000 per 1 mm3);
- the predominance of the concentration of leukocytes over the number of lymphocytes in percentage terms;
- opaque color of cerebrospinal fluid;
- low glucose levels;
- the presence of a bacterial focus of infection;
- positive reaction on Gram stain.
In typical types of the disease, the level of neutrophils reaches 75–95%. The leukocyte norm for newborns is up to 30/mm3. At an older age, the concentration should not exceed 5 leukocytes per 1 mm3. In healthy children who do not suffer from viral or bacterial meningitis, monocytes and lymphocytes predominate in the cerebrospinal fluid.
Tuberculous meningitis is characterized by specific symptoms:
- the lymphocyte content reaches 100/mm3;
- low glucose;
- bacterial foci determined by staining of the cerebrospinal fluid;
- cloudy liquid.
Deviations from normal indicators - video
In the presence of brain diseases, the cerebrospinal fluid changes its characteristics:
- If pathogenic microorganisms are present in it, it turns greenish-gray. A large number of leukocytes are found in the fluid.
- The red color of the cerebrospinal fluid indicates the presence of red blood cells. It happens with intense inflammatory damage or after injury.
- With the development of inflammatory processes in the body, the cerebrospinal fluid becomes yellow and even brown, and hemoglobin decomposition products are found in it. This condition is called xanthochromia.
- False coloration of the cerebrospinal fluid is also possible. It occurs with prolonged use of certain medications.
- The green color of the liquor occurs with purulent inflammation of the lining of the brain.
- A cyst rupture turns it dark.
- When protein elements are cytosed, the cerebrospinal fluid becomes opalescent.
- The disease process in the meninges increases the density of the spinal fluid to 1.015.
- Increased amounts of fibrinogen promote the growth of fibrosis clots and films. Typically, such phenomena occur during the development of the tuberculosis process.
Sometimes enzymes are found in the liquor. Normally, it should contain few enzymes. An increase in the content of these substances may indicate a disruption in brain activity.
With meningitis, counting the number of microbial cells is of particular importance . This number is critical for determining an accurate diagnosis and selecting a treatment method. The following calculation methods are used:
- determination of the number of cells that are stained using the Romanovsky Giemsa or Nokhtu method);
- counting liquor elements using a Fuchs and Rosenthal chamber. In its absence, a Goryaev chamber is used.
The increase in cells in the cerebrospinal fluid during meningitis is called pleocytosis. It is often diagnosed during inflammatory diseases. This phenomenon is most pronounced in the tuberculous form of meningitis.
Staining with Samson's solution makes it possible to accurately differentiate microbial and other cells. With meningitis, the number of lymphocytes, neutrophils, monocytes, eosinophils, and basophils increases. The doctor is interested in the quantity of all these elements.
Slow leakage of cerebrospinal fluid, the impossibility of obtaining it, pronounced coloring, discrepancy between the patient’s serious condition and the composition of the fluid, pronounced coagulation of the cerebrospinal fluid indicates that the patient is developing blocked types of meningitis.
The presence of atypical cells in the fluid while maintaining its transparency and the absence of increased protein content does not confirm the diagnosis of meningitis. The patient is referred for additional studies, since this sign may indicate the progression of a malignant process in the brain.
Indications and contraindications for the procedure
Lumbar puncture is prescribed in the following cases:
- signs of neuroinfection (encephalitis, meningitis and others);
- risk of hemorrhage in the subarachnoid space;
- clarification of the diagnosis of liquorrhea;
- diagnosis of oncological processes and metastases in the lining of the brain;
- diagnosis of cerebrospinal fluid fistulas using cerebrospinal fluid puncture and injection of contrast agent;
- diagnosis and prevention of neuroleukemia in patients with hematological oncology.
If there are such indications, taking a puncture of liquor fluid is the only and key diagnostic method. In some cases, the procedure is used as an additional examination method:
- diseases accompanied by destruction of the membrane of neurons of the central nervous system and PNS (demyelinating processes);
- inflammatory polyneuropathy;
- attacks of fever in the absence of other symptoms.
Contraindications
There are a number of contraindications to performing a lumbar puncture
However, in addition to the indications for puncture, there are also conditions whose presence requires abandoning this manipulation.
- Brain swelling. In this condition, lumbar puncture will lead to changes in intracranial pressure, which, in turn, can lead to herniation of the cerebellum into the foramen magnum and death. This is the most important and first contraindication to lumbar puncture.
- Any large-scale processes in the structures of the brain.
- Conditions with low blood clotting ability.
- Inflammatory conditions at the puncture site.
Risks and consequences of a spinal tap
Complications after puncture occur primarily when the rules of manipulation are not followed and doctors make mistakes. In other cases, the following consequences may occur:
- wedging of individual structural elements of the brain;
- dislocation of midbrain structures;
- damage to nerve endings causing pain in the patient;
- headaches, nausea, vomiting;
- hematomas at the site of needle insertion when small capillaries are damaged.
When taking cerebrospinal fluid material from pregnant women, the risk of spontaneous abortion increases, especially in the first third. Patients suffering from cardiovascular diseases also represent a risk group during manipulation. In particularly serious cases, the launch of vasovagal processes can provoke cardiac and respiratory arrest.
Contrary to popular belief that puncture can lead to paralysis, this complication is unlikely. The needle is inserted into the part of the spine that is most poorly innervated and the risk of damage to nerve endings is very low. The incidence of complications after puncture in patients does not exceed 1%.
After two weeks of intensive treatment, the patient’s health condition and the effectiveness of the chosen therapy method are assessed. To do this, repeat manipulation is performed with the collection of spinal fluid material for research. Based on the results of the puncture, changes in the cellular composition are analyzed and the presence or absence of a bacterial culture in the contents is determined. Positive dynamics indicate the patient’s clinical recovery.
Meningitis is a serious disease that requires accurate identification of the causative agent of the infection and the appointment of competent treatment. Cerebrospinal fluid puncture is the only and reliable method for diagnosing the disease.
Possible complications
If the procedure is carried out correctly, the risk of developing undesirable consequences is minimized, but there is a low probability of complications due to insufficient qualifications of the personnel or individual characteristics of the patient’s body. Such complications include:
- The appearance of hematomas at the puncture site. Hemorrhagic consequences can occur in the case of a poorly performed puncture due to damage to blood vessels or provoked bleeding.
- The occurrence of post-puncture syndrome. Complications occur due to displacement and dilation of blood vessels.
- Development of neoplasms in the spinal canal. Such consequences, accompanied by increasing pain in the lumbar region over time, can be caused by epithelial cells entering the spinal canal. This leads to the formation of epidermoid formations (tumors).
- The appearance of direct injury caused by an incorrectly inserted needle to collect cerebrospinal fluid. This complication is expressed in damage to nerve endings or damage to intervertebral discs. As a result, various infections may develop, and even another type of meningitis may occur.
- Changes in the cerebrospinal fluid sample due to the fact that during the collection of cerebrospinal fluid for research, the needle was inserted incorrectly, and air, particles of anesthetics, or chemical compounds could get into the sample.
- If there are violations during sample collection, radiculitis, myelitis or arachnoiditis may develop.
Sometimes, immediately after the puncture, symptoms such as severe dizziness, vomiting, and nausea may occur. This condition is associated with the characteristics of the patient’s body, it is not dangerous to health and disappears quickly enough if all the recommendations of specialists are followed.
2.Symptoms of meningitis
The most common symptoms of meningitis among teenagers and young adults are
:
- Tension and pain in the neck, especially when trying to touch the chin to the chest;
- Heat;
- Headache;
- Vomit;
- Convulsions;
- Drowsiness.
Signs of meningitis in children, the elderly and those with underlying health problems
, may be others:
- Babies may be fussy, cry and refuse to eat. They may develop a rash;
- Young children may feel like they have the flu. They may develop coughing and other breathing problems;
- Older adults and people with chronic illnesses may only experience a headache and fever with meningitis.
Visit our Therapy page
HIB-MENINGITIS: clinical picture, diagnosis and treatment
Meningitis caused by Haemophilus influenzae type B, or HIB meningitis, ranks third in frequency in the etiological structure of bacterial meningitis, accounting for 5 to 25% of cases. In the age group up to 4-5 years, this form of meningitis ranks second (from 10 to 50% of cases). In Moscow, in children under 5 years of age, HIB meningitis accounts for 15% of all cases of bacterial meningitis.
The incidence of HIB meningitis in children under 5 years of age before the start of routine vaccination in a number of countries varied from 23 cases per 100,000 children per year in developed European countries to 60 per 100,000 in developing countries. Before the introduction of vaccination against HIB infection, 370,000 cases of HIB meningitis were reported annually worldwide, of which about 100,000 were fatal (mainly in developing countries, which accounted for 97% of deaths). The mortality rate for this form of meningitis varies, according to various authors, from 5% (in developed countries) to 30% (in developing countries); Unfavorable long-term consequences are often observed.
Despite the significant place that HIB meningitis occupies in childhood infectious pathology, there are almost no works devoted to the pathogenic properties of the pathogen, pathogenesis and clinical features of this form of the disease. Publications devoted to the clinical aspects of HIB meningitis are based on a small number of observations and, as a rule, do not provide insight into the clinical and pathogenetic features of HIB meningitis.
Our report is based on an analysis of case histories of 89 patients with HIB meningitis, 71 of whom were treated in Clinical Hospital No. 2, 17 in other hospitals in Moscow. Observations cover the period from 1994 to 2001. Case histories of 150 patients with meningococcal meningitis, 51 with pneumococcal meningitis and 29 patients with meningitis of enteroviral etiology were used as comparison groups.
The diagnosis of HIB meningitis in 22 patients was confirmed after isolating a culture of the pathogen from the CSF or blood; in the other 22 patients, it was confirmed by latex agglutination. In 45 patients, the diagnosis was confirmed both bacteriologically and by latex agglutination.
As can be seen from table. 1, HIB meningitis is a disease of early and young childhood, and more than 11% of cases were children in the first 6 months of life (starting from 9 days), which indicates the absence or insufficiency of innate immunity. On the other hand, the fact that in children over 4 years of age, who belong to the most epidemiologically vulnerable age group, the incidence drops sharply can be explained both by the formation of acquired immunity (in children who have had various forms of HIB infection) and by age-related anatomical and physiological factors. characteristics of children of younger age groups.
Of the four patients over 8 years of age we observed, one child had a burdened premorbid background (exudative diathesis, multiple acute respiratory infections); two children aged 9 years suffered from purulent meningitis, of different etiologies, three to four times, which allows us to suggest the presence of an anatomical defect, most likely Spina bifida; Apparently, an adult woman suffered a skull injury, suffered from nasal liquorrhea and also repeatedly suffered from purulent meningitis of various etiologies.
HIB meningitis was severe in 88.6% of patients; in 12 patients the course of the disease was protracted (more than 2 months) or undulating. 6 patients died (6.7%).
From the data in table. 2 it follows that one of the important causes of mortality is hospitalization in non-core hospitals. This applies not only to patients with HIB meningitis, but also to patients with other neuroinfections.
Another reason is a burdened premorbid background: complicated pregnancy and childbirth, prematurity, organic damage to the central nervous system and other factors.
The third reason is late diagnosis and late hospitalization. The fourth is irrational therapy. Let's look at a typical case.
Patient U. from the Children's Home. Age - 1 year 3 months. He fell ill on February 27, 1997, was treated at the Children's Home for acute respiratory infections, and received ampicillin for the last day. On the 4th day of illness, the patient’s condition worsened and the patient was diagnosed with ARVI and pneumonia and was hospitalized at Children’s Infectious Diseases Hospital No. 12, where he received penicillin. On the 2nd day after hospitalization, the condition worsened, vomiting, muscle tremors, and bulging of the fontanel appeared. During puncture, purulent cerebrospinal fluid was obtained; the patient was transferred to clinical hospital No. 2 on the 6th day of illness. The condition upon admission was extremely serious. Upon repeated lumbar puncture, the diagnosis of purulent meningitis, complicated by cerebral edema, was confirmed. Concomitant disease: Down's disease, 3rd degree malnutrition. Treatment with penicillin was continued and intensive pathogenetic therapy was carried out. The patient's condition stabilized, but on the 3rd day it worsened again. Hyperthermia, convulsions, and loss of consciousness were observed. On the 3rd day of treatment, a culture of HIB was isolated from the CSF and blood, penicillin was replaced with chloramphenicol, but on the 5th day of treatment the patient died. On the day of death, the results of determining the sensitivity of the isolated culture were obtained: resistant to chloramphenicol and penicillin, sensitive to cefotaxime.
Pathological diagnosis: purulent meningitis caused by Haemophilus influenzae, cerebral edema, small-focal pneumonia. Associated complications: grade 3 accidental transformation of the thymus, Down's disease, grade 3 malnutrition, hydrocephalus.
This case illustrates the main causes of mortality: late diagnosis, severe premorbid background, inadequate antibacterial therapy. Nevertheless, thanks to rational pathogenetic therapy, death occurred only after 5 days, while in non-core hospitals all patients died within 24 hours, which, judging by the data of the case histories, is partly due to insufficiently adequate pathogenetic therapy. If we compare the mortality rate for purulent meningitis of various etiologies for the same period of time in the conditions of one medical institution (CIB No. 2), then for HIB meningitis it was 2.8%, for meningococcal meningitis - 6%, and for pneumococcal meningitis - 17%, i.e., in terms of prognosis for life, HIB meningitis is the most benign. At the same time, 8.5% of children were discharged with hearing loss, 13.4% with ataxia and other residual effects.
As can be seen from the above medical history, HIB meningitis often occurs against an unfavorable premorbid background, noted in 72% of patients. In most cases (62%), there were severe organic lesions of the central nervous system with hypertension and convulsive syndromes, developmental delays, paresis, etc. In patients with pneumococcal and meningococcal meningitis, the spectrum of background diseases was completely different, lesions of the central nervous system accounted for 12% and 3% respectively. Moreover, lesions of the central nervous system in pneumococcal meningitis were of traumatic origin. Frequent acute respiratory infections were observed in 52% of patients.
The onset of the disease in patients with HIB meningitis was acute, but the appearance of obvious clinical symptoms of meningitis was often preceded by moderate fever lasting from 1-2 to 5-7 days, accompanied by catarrhal symptoms from the upper respiratory tract. In 51% of patients, ARVI, pneumonia, catarrhal otitis, and sinusitis were initially diagnosed. In 6.8% of patients, fever was accompanied by dyspeptic symptoms, and they were diagnosed with acute intestinal infection.
Respiratory tract involvement is a characteristic manifestation of HIB infection, and it differs from those associated with meningococcal and pneumococcal infections. The absence of signs of meningitis in the early stages of the disease, as well as the underestimation of symptoms such as repeated vomiting, convulsive readiness, lethargy, and drowsiness, became the reason for the relatively late periods of hospitalization of patients.
Thus, in general, the average length of hospitalization was 3.1±0.17 days (for pneumococcal meningitis - 3.5±0.21 days, for meningococcal meningitis - 1.8±0.16).
The length of hospitalization of patients (Table 3) sent directly to Clinical Hospital No. 2 was 2.3 days, that is, they were significantly shorter. Naturally, this applies to children with the most striking clinical picture. More than half of the children were transferred to ICU No. 2 from other hospitals or were treated in them, most of them had problems with diagnosis. If hospitalization during the first two days of illness is conditionally considered timely, then it can be noted that 67.4%, that is, 2/3 of patients, were hospitalized in a specialized hospital during this period, while only 21.8% of patients were hospitalized in other hospitals. Thus, problems with diagnosing HIB meningitis lead to significantly later hospitalization of patients than with meningococcal meningitis. The duration of hospitalization affected not only the outcome of the disease, but also the duration of treatment. In hospitalized patients, in the first two days it was 25±0.3 days, after the 3rd day - 32.5±1.3 days (p<0.001). It should be emphasized that in general the duration of treatment was 27.7±0.9 days and was 8 days longer than for meningococcal meningitis.
What are the clinical features of HIB meningitis?
In addition to the anamnestic data mentioned above, upon admission to the hospital, 58% of patients were diagnosed with acute rhinitis and 87% with acute pharyngitis. The course of the disease was characterized by high fever lasting from 3 to 29 days, on average 11.8±0.9 days (Table 4), which is significantly longer than with meningococcal meningitis (8.4±0.7 days, p<0.001) , and approximately the same as with pneumococcal (13.5±0.9 days).
Moreover, there was not always a connection between the course of meningitis, the duration of fever and the timing of cerebrospinal fluid sanitization. The maximum level of fever varied from 37.8 to 41.3°C, averaging 39.6±0.08°C, that is, it turned out to be significantly higher than with meningococcal (39.2±0.07) and pneumococcal (39 .1±0.11) meningitis. In 53.9% of patients, fever ranged from 39.1 to 40°C, in 13.5% from 40.1 to 41.6°C, and in 4.5% up to 38°C.
In addition to the severity of the febrile reaction, the generalized nature of the infectious process in HIB meningitis is evidenced by the frequent enlargement of the liver (49%) and spleen (36%), as well as (in a large percentage of cases) the release of blood culture (44°C), and in the last two years blood cultures are isolated from almost all patients initially hospitalized in Clinical Hospital No. 2. For comparison: with meningococcal infection, the frequency of blood culture isolation was 16%, and with pneumococcal meningitis - 27%.
The nature and severity of CNS damage also differs compared to other common meningitis of bacterial etiology (Table 5).
Thus, HIB meningitis is characterized by a less severe course of the disease, a lower percentage of cases of cerebral edema, less profound and less prolonged disturbances of consciousness. Generalized convulsions were observed significantly less frequently. At the same time, focal convulsions and focal symptoms were more common, in particular cerebellar ataxia, damage to the cranial nerve, especially the VIII pair.
Meningeal syndrome was observed in almost all patients, but it was often expressed moderately, sometimes not fully. Thus, rigidity of the neck muscles was observed in 95% of patients, and Kernig’s sign and Brudzinski’s symptoms were observed in 74%; on average, meningeal syndrome regressed after 6.8 ± 0.4 days. The picture of the cerebrospinal fluid was similar to that of other purulent meningitis, but had some peculiarities. Pleocytosis above 1000 in μl was in 86% of patients, the content of neutrophils ranged from 70 to 100% (96.3±1.4%). Hyperproteinorachia was moderately pronounced, that is, most patients had a moderate increase in protein content (maximum up to 6.6 g/l), while with meningococcal and especially pneumococcal meningitis in severe cases this figure reached 9-12 g/l and even 30 g/l. On average, the protein level in HIB meningitis was 2.8±0.2 g/l, in meningococcal meningitis - 3.3±0.3 g/l, pneumococcal - 3.8±0.3 g/l.
The glucose content tended to decrease, averaging 1.7±26 g. However, in this case, the average indicator does not reflect the multidirectional nature of the change in this parameter. In more than 45% of patients, the glucose level was sharply reduced (less than 1 g/l) or glucose was not determined at all. This mainly concerned patients admitted late in the course of their illness. Upon early admission, 38% of patients had increased or normal glucose levels, that is, there were inverse relationships between the duration of hospitalization and glucose levels, which reflects the pathogenetic mechanisms on which this indicator depends: on the one hand, as a result of increased permeability of the BBB, the glucose content increases , on the other hand, the consumption of glucose by the pathogen leads to a decrease in its concentration. The same dependence is reflected by the dynamics of this indicator during the treatment process (Table 6).
Concluding the clinical characteristics of HIB meningitis, I would like to dwell on the features of the blood picture taking into account age standards (adults were excluded). The average age of the patients was 2.6±0.2 years. Leukocytosis was on average 13.1±1.17 thousand/μl, with leukopenia observed in 28% of patients, normocytosis in 21%, and normocytosis in half (51%) - leukocytosis. Leukocytosis over 15 thousand per μl was found in only 18.2% of patients, and the average value was only slightly higher than the norm. Even more demonstrative are the data on the number of lymphocytes, which reflects the state of the immune system. It varied from 300 to 5.5 thousand, and absolute lymphopenia was detected in 95% of children. Red blood, although to a lesser extent, indicated an unfavorable premorbid background. The hemoglobin level was also reduced and averaged 115.4±2 g/l. Normal hemoglobin levels upon admission were noted in 40% of patients; In 20% of patients, hemoglobin was below 100 g/l, that is, severe anemia was noted.
Initial therapy in 45 patients was carried out with benzylpenicillin at a dose of 200-400 thousand units/kg per day. After receiving the results of a bacteriological study or, in some cases, data on the sensitivity of the isolated strain to antibiotics, penicillin was replaced with other drugs. In 8 patients, treatment with penicillin was carried out for 4-8 days, after which the drug was replaced due to its ineffectiveness. In 3 patients, treatment was effective; its duration was 11, 14 and 16 days, respectively. Considering that in the younger age group, in addition to HIB, other flora resistant to penicillin (staphylococcus, group B streptococci, gram-negative flora) can also serve as an etiological factor for purulent meningitis, at present penicillin should not be used as a starting drug for purulent meningitis in children under 4-5 years.
In 18 patients, initial therapy was carried out with chloramphenicol-succinate; and in 9 of them it turned out to be ineffective. They replaced it with ceftriaxone. The duration of therapy ranged from 10 to 17 days, the effectiveness of chloramphenicol was 50%. Based on these data, it should be recognized that chloramphenicol is inappropriate to use for initial therapy.
Of the 14 patients treated with ceftriaxone or cefotaxime, 8 had an effect; in 6 cases, they were replaced with chloramphenicol, in one case with meronem, and in another with rifampicin.
When comparing the results of determining the sensitivity of the isolated HIB strains with the clinical effectiveness of treatment with cephalosporins, penicillin, chloramphenicol, it is obvious that the latter is 1.5-2 times lower (Table 7).
In total, of 19 patients who were treated with drugs to which the isolated HIB strain was sensitive, treatment was ineffective in 6 (32%). What are the reasons for this phenomenon? The following factors are likely to be relevant:
- low passage of antibiotics into the subarachnoid space or a rapid decrease in passage due to a decrease in the permeability of the BBB during treatment;
- the presence of zones of biological inaccessibility due to the anatomical age-related characteristics of the subarachnoid space in young children;
- disturbance of liquorodynamics in children with neurological background;
- unreasonable replacement of the drug due to the slow rate of cerebrospinal fluid sanitation.
As is known, β-lactam antibiotics pass through the BBB only in the presence of an inflammatory process, and as it subsides, the passage worsens. This phenomenon was described more than 40 years ago by V.I. Pokrovsky using penicillin as an example. In young children, the volume of the subarachnoid space in relation to body weight is 2-3 times larger, so the exchange of cerebrospinal fluid is slowed down, and accordingly, drug concentrations may be lower. In children with damage to the central nervous system, cerebral hydrops, cerebral hypertension, and partial occlusion of the cerebrospinal fluid pathways are often observed, which accordingly negatively affects the passage of drugs into the subarachnoid space.
Upon receipt of liquorological data indicating the presence of bacterial meningitis, initial therapy in children under 4-5 years of age should be carried out with ceftriaxone. If it is necessary to replace the drug, preference can be given taking into account data on sensitivity to chloramphenicol or benzylpenicillin, the dose of which we can increase to 500 thousand - 1 million / kg of weight, thereby achieving therapeutic concentrations. Preliminary experience also allows us to recommend fluoroquinolones and rifampicins according to individual indications.
To illustrate the above, we present the following case history.
Ganeeva Sarvinoz, 1 year 1 month, was in clinical hospital No. 2 from August 18 to September 15, 2001 with a diagnosis of purulent meningoencephalitis caused by M. inf. Atactic syndrome. Prolonged flow.
She was admitted to the department on the 5th day of the disease, which began gradually on August 14, with the temperature rising to 37.8°C. Became lethargic.
15.08 t = 39.5°C, appetite decreased. Examined by a local doctor. Diagnosis of ARVI.
In the following days, lethargy, drowsiness, and anorexia increased.
On August 18, headache and vomiting began. An emergency doctor admitted her to Children's Hospital No. 6 with a diagnosis of ARVI and meningeal syndrome. In the emergency department, chloramphenicol and prednisolone were administered intramuscularly, and the girl was transferred to clinical hospital No. 2.
Upon admission, the condition was severe, lethargic, loaded. The skin is pale. Muscle tone is reduced. No pathology was detected on the part of the cranial nerve.
Rigidity of the neck muscles, positive upper Brudzinski's sign, Kernig's sign, heart rate - 128 per minute, blood pressure - 90/55, respiratory rate - 24 per minute are pronounced. An LP was performed, which confirmed the presence of purulent meningitis.
19.08 - turbid liquor, C - 1797 liters in 1 mm3, B - 0.8%o. R-tion Pandi ++. The smear is 91% neutral. and 9% lymph. General blood test: Hb - 100, Er. - 3.9, L - 14.2, n - 30, S - 40, L - 27, M - 3, ESR - 48.
Upon admission, antibacterial therapy was carried out with chloramphenicol succinate 100 mg/kg.
On August 20, bacteriological confirmation of the diagnosis was received. HIB, sensitive to chloramphenicol, was isolated from the blood. Taking into account the ongoing fever, intoxication, the development of convulsive syndrome, an increase in blood leukocytosis to 25 thousand, and persistent pathological changes in the cerebrospinal fluid, chloramphenicol was replaced with longocef (100 mg/kg per day). The temperature returned to normal on the 10th day of treatment with Longocef, and cerebral and focal symptoms regressed. The seizures did not return. Lumbar puncture on August 29 and September 8 revealed lymphocytic pleocytosis. Subsequently, the patient’s condition was satisfactory and she was discharged home on September 15.
During the examination on October 16: cytosis - 21, protein - 0.3 g/l, smear - 100% lymphocytes.
This case illustrates the peculiarities of the course of HIB meningitis (late appearance of meningeal symptoms, prolonged fever against the background of effective antibacterial therapy and insufficient effectiveness of treatment with chloramphenicol, despite the sensitivity of the isolated HIB strain to it).
Table 2. Mortality in HIB meningitis
| Hospital | Number of patients | Died | Mortality, % |
| Profile | 79 | 2 | 2,5 |
| Non-core | 10 | 4 | 40,0 |
| Total | 89 | 6 | 6,7 |
back
Table 4. Duration of fever in HIB meningitis
| Number of units | Up to 5 days | 6-10 | 11-15 | 16-20 | More | Total |
| Abs. | 17 | 24 | 28 | 14 | 6 | 89 |
| % | 19,1 | 27,0 | 31,5 | 15,7 | 6,7 | 100 |
back