What is closed traumatic brain injury?
Closed skull trauma refers to all injuries to the skull and brain in which there is no damage to the scalp, and when a fracture occurs, the brain is not injured by the bone. That is, the intracranial cavity must remain closed.
Closed traumatic brain injury is injury to the head without compromising the integrity of the skin. In this case, there may even be a skull fracture, but the skin remains intact.
The severity of symptoms ranges from mild dizziness and nausea to the patient falling into a coma.
Any head injury is a strict indication to call an ambulance and transfer the patient under the supervision of medical personnel for early diagnosis and treatment of consequences.
Due to mechanical injuries, brain tissue is compressed, its layers move, and intracranial pressure rapidly increases. When displaced, damage to brain tissue and blood vessels often occurs, which results in changes in the biochemical composition in the brain with a deterioration in blood supply.
With clinical recovery after a traumatic brain injury, the long-term period is about 2 years; with a progressive course, the period is not limited.
If clinical symptoms do not disappear during this period and become stable, new neurological symptoms may appear.In people of the older age group, the acute period of TBI may be prolonged due to exacerbation of vascular and visceral pathology, the same can be said about long-term consequences.
Neurologist
Pershina Natalia Sergeevna
8 years of experience
Various changes occur at the cellular, tissue and organ levels. All this negatively affects the functioning of important body systems.
The blood flow to the brain worsens, the circulation of the cerebrospinal fluid changes, the barrier between the circulatory and nervous systems becomes thinner, which leads to the accumulation of fluid. As a result of the above changes, swelling of the brain is observed, which again leads to an increase in intracranial pressure.
Compression and displacement of brain structures can lead to infringement of the brain stem, which significantly impairs blood flow to the brain and reduces its active activity.
Recovery forecast
The success of restorative therapy and rehabilitation, therapeutic effects will largely depend on a huge number of specific factors:
- Nature of TBI.
- Severity of injury.
- Prompt provision of pre-medical first aid and professional medical care in a hospital setting.
- The quality of initial and general treatment and operations performed.
- Age of the patient (it is noted that infants and newborns and childhood victims have a much greater chance of successful rehabilitation than adults).
At the same time, the statistics do not take into account the described factors. Usually only the level of damage received is taken into account:
- Easy. If you have suffered a mild TBI, the prognosis will almost always be favorable, even if some functions were lost immediately after the injury (they are completely restored during the rehabilitation process). In situations where mild TBI is a recurring occurrence (for example, among those who practice martial arts), the risks of developing encephalopathy and dementia increase significantly.
- Average. In 90% of cases, the prognosis for moderate TBI is also quite optimistic, because 9 out of 10 patients recover within several months after injury. Typically, no more than 10% of victims receive disability.
- Heavy. A disease of this type is extremely dangerous to human health and life. The patient's health is seriously harmed. When receiving a severe traumatic brain injury, the mortality rate is 55% or higher. Almost all survivors (with rare exceptions) completely or partially lose their ability to work. When observing patients after treatment in intensive care and traumatology, they experience all sorts of disorders in the field of neurology and psychiatry.
In recent years, doctors at leading hospitals and institutes around the world (including in our country) have begun to differentiate injuries resulting from TBI into primary and secondary.
- A person receives primary damage directly at the moment of mechanical impact on the head (blow, fall, accident, etc.).
- Secondary damage does not develop in all cases, but quite often. Their manifestation is possible in case of illiterate first aid (including in intensive care, surgery), as well as in the case of a specific reaction of the patient to the damage that has occurred.
In cases where, after receiving a mild TBI, patients partially lose some functions (for example, hearing or coordination of movements) even after recovery and rehabilitation, the main reason for these negative processes is the occurrence of secondary rather than primary damage.
Secondary damage often occurs due to improper treatment or incomplete adherence by patients to the therapeutic course prescribed by doctors.
Classification
Closed skull injury is classified by severity into mild, moderate and severe:
- Mild degree (concussion, slight bruise). There is little or no direct trauma to the brain tissue, and 25% experience a skull fracture. Cardiac activity and respiration are normal. Neurological symptoms are mild and disappear after 15-20 days.
- With moderate severity, increased blood pressure and increased heart rate are possible, and mental abnormalities are not excluded. Symptoms of focal trauma appear (weakness of the limbs, changes in the pupil reflex). Fractures of the skull bones, hematomas and local lesions are often observed. With proper treatment, the development of pathological changes stops.
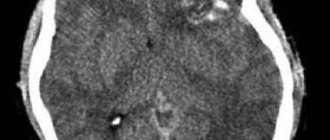
- In severe cases, large areas of the brain are affected; patients remain unconscious for a long time (several days) or fall into a coma. A tomography scan shows the presence of serious hematomas and skull fractures. Emergency surgery is often performed to remove hematomas.
Brain contusion
Brain contusion (CBM) is a type of traumatic brain injury.
According to clinical variants, the following types are distinguished: concussion, bruise, compression, diffuse damage:
- Concussion - occurs when struck by a blunt wide object, the skin often remains unharmed. Characterized by vomiting, dizziness, short-term loss of consciousness, amnesia.
- contusion (concussion) - some part of the brain is damaged, minor hemorrhages are possible, and sometimes tissue rupture is observed. The patient loses consciousness, and upon restoration of consciousness, neurological changes are noted. Speech dysfunction, convulsions, coma are possible.
- Compression of the brain - observed with the development of edema, pressing of the bone into the skull, and effusion of blood. Headache, nausea, and heart failure develop.
- Diffuse damage is the most severe condition, coma for up to a month, after leaving it the patient often cannot recover for the rest of his life, since there have been severe deviations in the functioning of the cerebral hemispheres (vegetative state).
Complications of TBI
Open head injuries have many complications, and they can be both early and late. Negative consequences must be eliminated, as they can lead to disability or death of the patient.
Complications:
1. Non-infectious (early). They are directly related to the injury itself:
- Bleeding and hemorrhage. This is the earliest complication that occurs immediately after injury. Bleeding may be profuse. In the presence of hemorrhage, there is an increase in neurological symptoms and a sharp decrease in vital signs.
- Shock. This complication is not common with open head injuries. It occurs if the patient has multiple injuries or massive blood loss.
- Liquorhea is the leakage of cerebrospinal fluid outward. This condition can lead to the development of meningitis.
- Brain prolapse. As a rule, this pathological condition develops within the first 30 days from the moment of injury. The protrusion can be of various shapes and sizes.
2. Infectious (late). They arise due to infection that enters the wound:
- Meningitis and meningoencephalitis. If the wound is treated poorly, then soft tissue infection occurs in its area. The infection then enters the wound canal and spreads to the meninges. With deep penetration of pathogenic microflora, encephalitis with corresponding symptoms joins meningitis.
- Infectious lesion of the wound channel. This can lead to the occurrence of liquor leaks and fistulas, as well as osteomyelitis (if the skull bones are affected by infection).
- A brain abscess is the presence of a cavity filled with pus in a major organ. It forms at the site of hematomas, around inert debris and foreign bodies that have entered the brain tissue through the wound canal.
- Adhesions and the formation of calluses and scars.
- Convulsive syndrome. Convulsions can be single or serial, and also have the nature of status epilepticus.
Causes
The main factors that provoke closed traumatic brain injury:
- Accidents on the road (pedestrians and drivers may become victims).
- Various falls from heights.
- Beating.
- Sports and household injuries.
- Industrial injuries.
In modern times, young people are more likely to experience criminal injuries that were sustained while drunk or under the influence of drugs.
Older people mostly suffer when they fall from their height.
The number of accident victims increases in early autumn and winter.
Symptoms
After an injury, signs may appear immediately or after some time, it all depends on the injury itself and its severity:
- Loss of consciousness occurs immediately after the injury. The time spent without consciousness can last several hours, in more complex situations it can be several days. At this time, the patient does not respond to external stimuli and does not feel pain.
- Headache – begins immediately after regaining consciousness.
- Nausea and vomiting do not give a feeling of relief.
- Dizziness.
- Redness of the face and neck.
- Increased sweating.
- Hematoma - most often occurs with fractures of the bone frame of the skull. You can often observe the ear and near the eyes.
- Leakage of liquor fluid through the ears or nose (indicates damage to the integrity of the lining of the brain by a piece of bone).
- Development of convulsive limb syndrome, often in an unconscious state, tongue biting and involuntary urination.
- Amnesia - a person does not remember events that happened before the injury (occasionally there are cases when a person forgets events that happened after the injury).
If the vessels of the brain are damaged, then hemorrhage in the membranes is possible. This situation is manifested by the following symptoms:
- A sudden headache .
- Photophobia is pain in the eyes in bright light.
- Vomiting and nausea that do not make you feel better.
- Loss of consciousness.
- The muscles of the back of the head are tense, which is characterized by a head thrown back.
If a certain part of the brain is damaged (focal lesion), then the symptoms will depend on its location.
Frontal lobe:
- Speech impairment (slurred and unintelligible speech).
- Gait disturbance (a person may fall on his back).
- Weakness in the arms and legs (either the right or left limbs suffer).
Temporal lobe:
- Speech disorder (a person ceases to understand the speech of other people, although he hears well).
- Some parts of the visual field are missing (drop out).
- Convulsive seizures.
Parietal lobe - unilateral loss of sensitivity of the body (cannot feel touch, pain, sudden changes in temperature), either the left or the right side is affected.
Occipital lobe - partial or complete loss of vision (sometimes loss of the visual field).
Cerebellum:
- Loss of coordination of movements (body movements are rough and sweeping).
- Unsteadiness of gait (“drunken gait”; falls are possible).
- nystagmus .
- Muscle tone is significantly reduced.
If the nerves are damaged, strabismus, facial asymmetry (curvature of the lips, different eye shapes), and hearing impairment may occur.
Signs may differ according to clinical variants:
- Concussion - loss of consciousness, nausea and vomiting, amnesia. No neuralgic abnormalities are observed.
- contusion - symptoms similar to concussion. The bruise can be detected at the site of the impact and on the impact side (opposite). Loss of consciousness lasts from two to three minutes to an hour.
With a slight bruise, the patient complains of a headache, nausea, vomiting; when looking to the side, the eye begins to twitch; on one side of the body, muscle tone is higher than on the opposite. When analyzing cerebrospinal fluid, an admixture of blood is sometimes observed.
Why can our articles be trusted?
We make health information clear, accessible and relevant.
- All articles are checked by practicing doctors.
- We take scientific literature and the latest research as a basis.
- We publish detailed articles that answer all questions.
With a moderate injury, the unconscious state can last up to several hours. Amnesia, vomiting, and headache are observed. Breathing, heart function, blood pressure are impaired, and a mental disorder is possible. The pupils may be of different sizes, speech is unintelligible, general weakness. Significant admixture of blood in the cerebrospinal fluid. Fractures of the vault and base of the skull are often found.
In severe cases, unconsciousness lasts several days. Breathing, heart rate, blood pressure, and body temperature are impaired. Sometimes seizures and paralysis occur. The most common structural fractures of the skull with hemorrhages are:
- When the brain is compressed, a hematoma is observed. In a milder case, the patient has complete apathy and lethargy. In severe situations - falling into a coma. A large hematoma is often accompanied by a tentorial hernia, which compresses the brain stem; against this background, damage to the optic nerve and cross paralysis of the legs and arms occurs.
- fracture is always accompanied by brain contusions, blood from the skull penetrates the nasopharynx, eye shell, middle ear, and sometimes there is a violation of the integrity of the eardrum.
- The discharge of blood through the nose and ears may indicate a local injury and the “symptom of glasses”; sometimes there is a leakage of cerebrospinal fluid, especially when the head is tilted forward.
- A fracture of the temporal bone is quite capable of causing paralysis of the auditory and facial nerves, and sometimes this manifests itself after some time.
Sometimes alcoholics and the elderly experience a chronic hematoma; usually the injury is not severe and is forgotten by the patient.
Diagnostics
Diagnosis of a skull injury begins with a medical history, which is based on a complete examination of the patient and his complaints (head pain, dizziness, general malaise, etc.). Next, diagnostics are carried out to establish the neurological condition, analyze breathing and heart function.
If alcohol intoxication is suspected, tests are performed to confirm its presence in the blood, urine and cerebrospinal fluid (the fluid that bathes the brain). However, all this does not give a complete assessment of the picture, so the following diagnostic methods are prescribed:
- An X-ray of the brain is performed
- Carrying out computed tomography and magnetic resonance imaging, which is considered a more accurate indicator.
- Measurement of general and intracranial pressure.
- Puncture of cerebrospinal fluid - according to indications.
- Angiography is a study of cerebral vessels with the introduction of contrast agents.
A positive prognosis for the victim can only be ensured by timely and correct diagnosis along with properly selected treatment. This combination can block the development of complications and eliminate the consequences.
Treatment
Treatment for closed skull trauma depends on the type of injury sustained.
Self-medication is dangerous with complications!
Attention
Despite the fact that our articles are based on trusted sources and have been tested by practicing doctors, the same symptoms can be signs of different diseases, and the disease may not proceed according to the textbook.
Pros of seeing a doctor:
- Only a specialist will prescribe suitable medications.
- Recovery will be easier and faster.
- The doctor will monitor the course of the disease and help avoid complications.
find a doctor
Do not try to treat yourself - consult a specialist.
In case of a concussion, the victim should be placed on a horizontal surface with his head slightly raised. If you are unconscious, lie on your right side, your left arm and leg should be bent - this will make breathing easier. Turn your face toward the ground to prevent your tongue from sticking and vomit and blood from getting into your respiratory tract.
Next, the patient must be placed for inpatient treatment, if no focal lesions are found and if the patient is feeling normal, it is allowed not to carry out drug therapy, and the patient is transferred to outpatient treatment. Therapy is aimed at stabilizing the functioning of the brain and eliminating symptoms; for this purpose, analgesics and sedatives are prescribed (usually in tablets).
If there is a disturbance of consciousness less than eight points on the Glasgow scale, artificial ventilation is required.
To normalize intracranial pressure, hyperventilation, as well as medications from the barbiturate group, are prescribed. To avoid complications, antibacterial therapy is used. To eliminate convulsive seizures - anticonvulsants.
Surgical intervention is used for the development of an epidural (between the skull and the membrane) hematoma with a volume of 30 cm³ or more, as well as for a subdural (between the membranes of the brain) hematoma, the thickness of which exceeds 10 mm.
Urgent Care
Emergency assistance is provided directly at the scene of the incident. It is carried out by medical workers. Algorithm for providing first aid to a victim:
- Stop bleeding and apply an aseptic dressing to the wound.
- If cardiac and respiratory functions are impaired, artificial ventilation and indirect cardiac massage are performed. In some cases, an injection of adrenaline is given.
- It is necessary to hospitalize the patient as soon as possible. Its transportation is carried out only after immobilization (the head must be securely fixed).
- Monitoring the condition of the victim during transportation.