Aneurysm is an insidious disease that is rarely accompanied by clinical signs and is usually discovered by chance.
This is a pathology in which the wall of the artery bulges due to stretching or thinning. In this case, the lumen of the vessel expands more than 2 times. Theoretically, this can occur in any artery, but the largest ones are most often affected.
Its complete removal can only be done surgically. Below we will discuss the indications for surgery and modern methods of treating pathology.
How the condition develops
At the site of aneurysm formation, the walls of the vessel lose elasticity, weaken and cannot resist the flow of blood. As a result, a protrusion is formed, a kind of sac filled with blood. If the aneurysm is small in size and does not manifest itself with symptoms, a person may not be aware of its presence in the brain. Gradually increasing, one day its integrity is violated. The weak point is the apex, where the rupture occurs, causing a hemorrhagic stroke.
The duration of bleeding lasts seconds, but this is enough to cause damage to the brain. Usually the body quickly reacts to a violation of the sealing of blood vessels. A reflex spasm of the adductor artery occurs, the formation of blood clots at the rupture site increases, which leads to stopping the release of blood and thereby saving a person’s life. When the process is delayed and bleeding continues, death occurs.
Methods used in surgery
There are several ways to remove an aneurysm: which one is more preferable is determined by the doctor individually. This depends on the location of the pathology, the size of the lesion, the individual characteristics of the body and the presence of concomitant diseases.
Surgery for an aneurysm can be:
- Palliative – surgeons create conditions under which thrombosis and desolation of the aneurysm develop. However, such interventions are not very effective and often lead to relapses. Therefore, they are used only when other methods cannot be used.
- Exclusion of the aneurysmal sac from the circulatory system - ligature operations.
- Restorative interventions during which vascular patency is partially or completely preserved.
Reconstructive operations for aneurysms are performed most often and are considered the most effective.
Reasons for the breakup
Arterial wall weakness is often genetic. Sometimes renal pathologies, injuries, oncology, and atherosclerosis lead to the occurrence of a cerebral aneurysm. What factors contribute to the violation of the integrity of the vascular wall:
- increased physical activity;
- arterial hypertension;
- emotional stress;
- drinking alcohol;
- infectious diseases accompanied by high fever.
When a rupture occurs, blood flows into the anatomical space or directly into the brain, putting pressure on the tissue, which is manifested by signs characteristic of cerebral hemorrhage.
When is surgery necessary for cerebral aneurysm?
cerebral aneurysm
A strict approach is necessary to the rationale for surgical intervention for an unruptured aneurysm due to possible complications during the operation. Aneurysms larger than 7 mm are considered indications for surgery. Indications for surgery become more specific as the aneurysm increases in size over time and with a family predisposition to hemorrhage (cases of hemorrhage from an aneurysm in close relatives).
Symptoms
When there is a threat of rupture, some (up to 15%) patients develop nonspecific symptoms within 1–5 days: widespread headache, focal neurological manifestations associated with the location of the aneurysm, and sometimes seizures. Therefore, when a person knows about the pathology, if the condition changes, it is better to immediately consult a doctor.
But more often, a hemorrhagic attack begins unexpectedly. The clinical picture of what is happening depends on the amount and speed of the blood being shed and the area where the damage occurred:
- Among the first manifestations, an intense headache stands out; it comes suddenly and is compared by patients with a sharp blow to the head. More often it involves the entire head, sometimes it is local in nature.
- After a few seconds, dizziness occurs and vomiting occurs.
- Often, the pain syndrome may be replaced by confusion or loss of consciousness. The condition can last 20 minutes, sometimes several hours, and sometimes a coma develops.
- Upon returning to consciousness, the patient is weakened, dizzy, and has poor orientation.
- Autonomic disorders are accompanied by rapid breathing (up to 20 times per minute) and an increase in heart rate.
- Neurological manifestations are expressed in severe stiffness of the neck muscles, impaired oculomotor functions, tremors, paresis, loss of speech functions and paralysis. Generalized seizures are observed in 10% of patients.
- With a hematoma in the area of the thermoregulatory center, persistent hyperthermia develops.
- In some cases, mental disorder and disorientation in space are observed.
The general condition is serious and requires immediate medical attention.
With minor hemorrhages, when a tear occurs or microcracks form in the wall of the aneurysm, a small amount of blood enters the brain. In this case, the symptoms are blurred, pass without loss of consciousness and vomiting with a slight increase in temperature.
First aid
If an aneurysm rupture is suspected, urgent hospitalization is necessary. But in some situations, when characteristic symptoms appear, a person needs help immediately, otherwise the risk of death is high. What needs to be done before the doctors arrive:
- The patient is laid horizontally, the head should be in an elevated position. This is necessary to ensure the outflow of venous blood and reduces the risk of developing severe cerebral edema.
- A person needs to ensure a flow of oxygen; to do this, unbutton the top buttons on his clothes and untie his tie. This will help improve blood supply to the brain, reduce hypoxia, and delay the death of neurons.
- In case of loss of consciousness, the airways should be cleared: dentures are removed, the head is turned to the side to prevent inhalation of vomit.
- To reduce the spread of swelling and hemorrhage in the head, cold objects are applied. Whatever you have on hand, any bag from the refrigerator will do. Cold promotes vasoconstriction and accelerates the process of blood clotting.
Manipulations do not always help with extensive hemorrhages; often the patient dies in the first minutes of an attack. But you should fight for a person’s life until the ambulance arrives. Urgent measures will help reduce the amount of irreversible changes and save his life.
Diagnostics
When a patient with an aneurysm is admitted to the hospital, diagnostic tests are performed:
- A physical examination is necessary to determine the severity of the patient's condition, autonomic and neurological disorders. It is difficult to accurately diagnose a rupture using this method, but a decrease in blood pressure indicates hemorrhage.
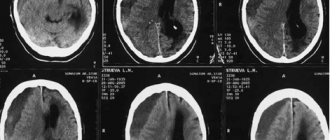
- Computed tomography, the main method for diagnosing a ruptured aneurysm, provides an image of the brain using X-rays and an electromagnetic field. The study makes it possible to see the location of the vessels and identify the area and volume of the pathological focus. In cases where the hemorrhage is located in the subarachnoid space, aneurysm rupture can be diagnosed. But this device is not available in every hospital, so it is not always available.
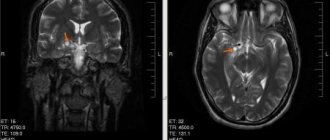
- Cerebral angiography is used more often and is an x-ray examination using a contrast agent. The procedure will indicate the location, shape and size of the aneurysm, and the extent of the damage. The classic technique involves inserting a catheter into the groin area. In spiral angiography, a substance is injected into a vein.
- Lumbar puncture is performed by puncturing the spinal canal, collecting cerebrospinal fluid and performing liquorodynamic tests. If there is venous blood in the brain fluid, the presence of hemorrhage in the brain is determined.
The examination helps to differentiate aneurysm rupture from other pathologies, determine the degree of destructive changes in the brain, and choose the most appropriate treatment tactics to stabilize the condition.
Treatment
Treatment of an aneurysm aims to prevent re-bleeding and the consequences of rupture. The main method is surgery. The doctor chooses the method of surgical intervention depending on:
- location of the aneurysm;
- patient's condition;
- severity of violations;
- the time interval that has passed since the break.
What types of operations exist:
- Clipping. The microsurgical method is used most often and involves clamping the base or body of the aneurysm with a clip to isolate it from the bloodstream without violating its integrity. Manipulation requires craniotomy, so the operation is considered the most difficult, but allows direct access to the damaged area. Open intervention is also used when wrapping muscles or surgical gauze around a damaged vessel to strengthen it.
- Endovascular method. The method does not involve opening the skull; it is carried out using a catheter through the femoral artery. Next, the tube is pushed through the vessels into the brain to the damaged area of the artery. At the end there is a spiral, with the help of which the protrusion is closed. Subsequently, it thromboses, preventing the cavity from filling with blood. During the operation, the surgeon monitors the process using an X-ray machine. Sometimes the artery is completely soldered, and nutrition is supplied to the brain tissue bypassing other vessels. The advantage of the method is that it is gentle on the body, so complications occur less frequently and the patient will need less time for rehabilitation.
- The combined method involves first introducing a blood clot into the aneurysm, then clipping it.
It is important to perform the operation no later than 72 hours after the start of bleeding, as the risk of relapse is high. Over time, due to destructive processes, vasospasm increases, ischemia develops, and the operation becomes useless.
After operation
Complications are common after surgery. Each type of intervention has its own consequences:
- After cleaning, the normal circulation of cerebrospinal fluid is disrupted, the nerve centers of the meninges are irritated, and swelling is present at the trepanation site. As a result, in the postoperative period, disturbances in balance, vision, hearing may occur, and the person may experience headaches. Typically, such manifestations are rare and temporary.
- Endovascular intervention carries its own risks: sometimes the aneurysm ruptures again at the time of surgery, and it may be perforated by a coil. If the implant is placed incorrectly, it is possible that it will dislodge and fill the protrusion with blood. There is also a danger of blood clots forming and blocking a vessel located after the area where the coil is placed.
Death also occurs after surgery, when the brain damage is extensive or help is provided too late.
Conservative treatment
Therapeutic treatment is prescribed for minor defects or when surgical manipulations cannot be performed. The patient is required to follow all doctor's instructions and adhere to bed rest. Treatment is used to lower blood pressure, dilate blood vessels and remove fluid from brain tissue. Medicines that increase blood viscosity are also used. Therapy alleviates the patient's condition, but does not guarantee that the hemorrhage will not recur.
Complications after a rupture
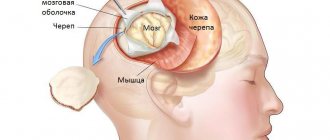
The anatomical location of the aneurysm is the subarachnoid cisterns, so at the moment of rupture, blood fills the subarachnoid space. This is a specific manifestation of protrusion rupture. Within 20 seconds, the blood spreads throughout the entire area, and after a few minutes it penetrates the spinal cord. Therefore, death occurs in 15% of cases even before the doctors arrive, and half of the patients die in the hospital.
Intracerebral hemorrhage occurs when a hematoma forms inside the brain, which is observed in 15% of episodes, 5% belong to situations where blood is poured into the ventricular system. In this case, they fill with liquid, which causes death.
What happens in the brain after a rupture:
- Spilled blood sometimes clogs the cerebrospinal fluid drainage pathways, which leads to fluid accumulation, cell hypoxia and the development of hydrocephalus, and displacement of brain structures.
- After a stroke, the blood forms a hematoma, and when it breaks down, toxic substances are released. Inflammation develops and tissue necrosis occurs in the brain.
- Complications include vasospasm - a sharp narrowing of blood vessels, which leads to a deterioration in cerebral blood supply. If in the first seconds this factor works to stop bleeding, it subsequently leads to cerebral ischemia and ischemic stroke.
After a rupture, the affected area of the brain stops working. If the patient remains alive, pathological changes in tissues disrupt the functioning of organs and systems. The degree and forms of severity are determined by the volume and localization of destruction, ranging from minor manifestations to complete paralysis. What are the most common consequences:
- Cephalgia. The pain syndrome is not relieved by analgesics.
- Paralysis and paresis. People who have suffered a rupture of an aneurysm experience disturbances in the motor system, paralysis of a part of the body (hemiparesis), and complete paralysis.
- Speech. Hemorrhage in the left hemisphere causes difficulties with writing and reading, reproduction and perception of speech. Natural acts. Sometimes a person loses the ability to swallow food and inhales its particles, which can lead to inflammation in the respiratory system or death from asphyxia. It happens that control over the sphincters is lost, constipation or urinary retention develops.
- Mental pathologies. The patient's behavior changes: he becomes aggressive and has bouts of rage. In some cases, apathy and depression occur. The disorder manifests itself in inappropriate behavior and mood instability.
- Cognitive abilities. Disturbances also affect thinking abilities: memory suffers, a person does not remember events, does not perceive new information, and his perception is distorted.
- Epilepsy. Epileptic seizures of a local or generalized nature develop.
A re-rupture cannot be ruled out. Usually the next stroke is more severe than the first.
Rehabilitation
After a hemorrhagic stroke and postoperative complications due to damage to brain cells, a person loses some functions; a quarter of patients are unable to care for themselves throughout the year. To eliminate the consequences, rehabilitation measures are required:
- Positional treatment is used early on for patients with paralysis. To reduce muscle tension in the limbs and improve blood circulation, they are laid down for an hour or two in such a way as to reduce the load. For fixation, special splints are used.
- For paralysis, massage the limbs and collar area.
- Physiotherapeutic procedures are used.
- Special classes are conducted for disorders of the hearing and speech apparatus.
- Attention is paid to the development of fine motor skills.
- Physical therapy and training on simulators are widely used.
All procedures are performed strictly according to the doctor’s recommendation. An individual scheme of measures is developed for each patient. During a difficult period, the attention and care of loved ones is important; only their support will help a person recover.
The main prevention of cerebral aneurysm rupture is regular examinations. To prevent the tragic outcome of events and reduce the risk of developing severe consequences, it is necessary to regularly monitor the condition of blood vessels. You should streamline your daily routine, balance your diet towards a healthy diet, and avoid smoking and drinking alcohol.
How long do they stay in the hospital with a stroke, depending on the type of illness?
In severe forms of stroke, a disability is often assigned, and the person is released from his usual work. A medical and social examination must establish and assign a disability group. It should be noted that patients after a rupture of an aneurysm leading to a hemorrhagic stroke remain in intensive care for at least 60 days . After this, they receive sick leave for at least 4 months.
After a stroke, the patient is kept in the intensive care unit for no more than 3 weeks after the attack. During this period, doctors take care that serious complications do not arise due to the improper functioning of certain systems, mainly the brain. All patients are hospitalized, regardless of the form of hemorrhage. The length of stay in a clinical setting depends on the following factors: