The role of the neocortex in emotions and stereogynesis
Emotions in humans initially appear in the limbic system of the brain. But in this case they are represented by primitive concepts, which, once in the new cortex, are processed using the associative function. As a result, a person can operate with emotions at a higher level, which makes it possible to introduce concepts such as joy, sadness, love, anger, etc.
The neocortex also has the ability to dampen strong outbursts of emotion in the limbic system by sending calming signals to areas of high neuronal excitability. This leads to the fact that in a person the dominant role in behavior is played by the mind, and not by instinctive reflexes.
PHYSIOLOGY OF THE CEREBRAL CORTEX
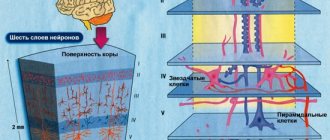
A. Structural and functional organization of the cortex. The cerebral cortex is a multilayered neural tissue
with many folds.
The cortex has 6 layers (I-VI), each of which consists of pyramidal and stellate cells
(Fig. 5.16). The main feature of pyramidal cells (the name reflects the shape of the cells) is that their axons extend from the cortex and also terminate in other cortical structures. The name of stellate cells is also due to their shape; their axons end in the cortex, i.e. we are talking about cortical interneurons. In layers I-IV, perception and processing of signals entering the cortex in the form of impulses occur. The efferent pathways leaving the cortex are formed mainly in the V-V1 layers. The division of the cortex into various fields was carried out by K. Brodmann (1909) on the basis of cyto-architectonic features - the shape and location of neurons. The author identified 52 fields, many of them are characterized by functional and neurochemical features.
Corticalization of functions -
an increase in phylogenesis of the role of the cerebral cortex in the analysis and regulation of body functions and subordination of the underlying parts of the central nervous system. Switching off the cerebral cortex in monkeys and humans leads to the loss of not only locomotion, but also righting reflexes, which are preserved in other mammals.
B. Localization of functions in the cerebral cortex. In certain areas of the cerebral cortex, neurons are concentrated that perceive a certain type of stimulus: light - the occipital region, sound - the temporal lobe, etc. Motor functions are also distributed over large areas of the cerebral cortex, for example, neurons whose axons form the pyramidal tract are located not only in the motor areas, but also beyond them. Currently, the division of the cortex into sensory, motor and associative (nonspecific) zones is accepted.
Sensory areas of the cortex -
these are the zones that receive sensory information (from receptors): the projection cortex, the cortical sections of the analyzers according to I. P. Pavlov.
These zones are located mainly in the parietal, temporal and occipital lobes. The ascending pathways to the sensory cortex come primarily from the relay sensory nuclei of the thalamus. Primary sensory areas are
zones of the sensory cortex, irritation or destruction of which causes clear and permanent changes in the sensitivity of the body (analyzer nuclei according to I.P. Pavlov).
They consist predominantly of monomodal neurons and form sensations of one quality (one modality). In the primary sensory zones there is usually a clear spatial (topographic) representation of body parts and their receptor fields. Around the primary sensory zones there are less localized secondary sensory zones, the neurons of which respond to the action of several stimuli, i.e.
they are multimodal. The most important sensory area is the parietal cortex of the postcentral gyrus and the corresponding part of the paracentral lobule on the medial surface of the hemispheres, which is designated as somatosensory area I. Here there is a projection of skin sensitivity on the opposite side of the body from tactile, pain, temperature receptors, interoceptive sensitivity and sensitivity musculoskeletal system - from muscle, joint, tendon receptors (Fig. 5.17).
In addition to somatosensory area I, there is a smaller somatosensory area II, located on the border
Motor cortex areas.
There are primary and secondary motor areas.
In the primary motor cortex (precentral gyrus, area 4) there are neurons that innervate the motor neurons of the muscles of the face, trunk and limbs.
It has a clear topographic projection of the muscles of the body (see Fig. 5.17). The main pattern of topographic representation is that the regulation of the activity of muscles that provide the most accurate and varied movements (speech, writing, facial expressions) requires the participation of large areas of the motor cortex. Secondary motor cortex
(field 6) is located both on the lateral surface of the hemispheres, in front of the precentral gyrus (premotor cortex), and on the medial surface, corresponding to the cortex of the superior frontal gyrus (supplementary motor area).
In functional terms, the secondary motor cortex has a dominant role in relation to the primary motor cortex, carrying out higher motor functions associated with planning and coordination of voluntary movements. readiness potential, which occurs approximately 1 s before the start of movement,
is most recorded The cortex of area 6 receives the main part of the impulse from the basal ganglia and the cerebellum and is involved in the recoding of information about the plan of complex movements. Association cortical areas
(synonyms: nonspecific, intersensory, interanalyzer cortex) include areas of the new cerebral cortex that are located around the projection zones and next to the motor zones, but do not directly perform sensory or motor functions - they cannot be attributed predominantly sensory or motor functions, the neurons of these zones have great learning abilities.
The boundaries of these areas are not clearly defined. Neurons of the associative cortex are polysensory (polymodal): they respond, as a rule, not to one (like neurons of the primary zones), but to several stimuli - the same neuron can be excited by irritation of auditory, visual, skin and other receptors. As a result of this, the associative cortex is a kind of collector of various sensory excitations, participates in the integration of sensory information and in ensuring the interaction of sensory and motor areas of the cortex.
Currently, based on thalamo-cortical projections, two main associative systems of the brain are distinguished: thalamo-parietal and thalamo-frontal. There is an opinion about the advisability of isolating a third system, the thalamotemporal system. Section II
PHYSIOLOGY OF INTERNAL ORGANS AND BODY SYSTEMS
Chapter 6 BLOOD SYSTEM
The blood system is a combination of hematopoietic organs, peripheral blood, blood destruction organs and the neurohumoral regulatory apparatus (G. F. Lang).
Check-up at the Central Clinical Hospital of the Russian Academy of Sciences. Fast, efficient, inexpensive
Experienced doctors of the Central Clinical Hospital of the Russian Academy of Sciences use modern diagnostic methods and the latest medical equipment in their work. Those wishing to check their health in our clinic can independently choose the day of the examination.
Check-up “Headache” at the Central Clinical Hospital of the Russian Academy of Sciences is not only pictures, test results and medical reports. Each patient receives professional recommendations from qualified doctors, and, if necessary, can undergo outpatient or inpatient treatment in our clinic.
To register for an examination at the Central Clinical Hospital of the Russian Academy of Sciences and clarify the cost of services, you can call or use a special form on the website.
Causes and consequences of headaches
To get rid of headaches caused by ordinary overwork, it is enough to get a good night's sleep, adjust your lifestyle and diet. But this does not help in all cases, just like taking pills in an attempt to numb the pain. If painful sensations in the head are caused by developing pathological processes, it is necessary to identify and eliminate their causes. It can be:
- hormonal disbalance;
- vascular diseases;
- neurological disorders;
- viral diseases;
- inflammation of ENT organs;
- cranial injuries and post-traumatic pathologies;
- tumor processes.
A specially designed check-up program will help you find out what triggers your headache. Many diseases can develop for years without any symptoms. The examination results in such cases come as a complete surprise to patients.
How to do a Check-up for complaints of headaches
The Check-up examination program includes the following procedures:
- daily observation;
- MRI of the brain and one part of the spine;
- duplex/triplex scanning of extracranial sections of the brachiocephalic arteries;
- radiography of one part of the spine with functional tests;
- 24-hour blood pressure monitoring;
- electroencephalography;
- ECG;
- blood test for 10 indicators and urine test.
Consultations are carried out by a neurologist and an ophthalmologist. During the final conversation, the patient is introduced to the detailed results of the examination and is given a medical report with recommendations for prevention or treatment. If necessary, additional examinations are prescribed.
| CheckUp Headache program | ||||
| The program includes: | ||||
| B01.023.001 | Primary appointment (examination, consultation) with a neurologist | 1 500 | 1 | 1500 |
| В01.023.002 | Repeated appointment (examination, consultation) with a neurologist | 1 200 | 1 | 1200 |
| B01.029.001 | Primary appointment (examination, consultation) with an ophthalmologist | 1 700 | 1 | 1700 |
| A05.23.009 | Magnetic resonance imaging of the brain | 5 760 | 1 | 5760 |
| A05.03.002 | Magnetic resonance imaging of the spine (one section) | 5 760 | 1 | 5760 |
| A04.12.005.005 | Duplex/triplex scanning of extracranial sections of the brachiocephalic arteries | 3 000 | 1 | 3000 |
| A06.03.019 | X-ray of the spine with functional tests (one section) | 2 000 | 1 | 2000 |
| А02.12.002.001 | 24-hour blood pressure monitoring | 3 500 | 1 | 3500 |
| A05.23.001 | Electroencephalography | 2 000 | 1 | 2000 |
| А11.12.009 | Taking blood from a peripheral vein | 250 | 1 | 250 |
| B03.016.002 | General (clinical) blood test (hemoglobin, leukocytes, platelets, erythrocytes) | 320 | 1 | 320 |
| A09.05.010 | Study of the level of total protein in the blood | 190 | 1 | 190 |
| A09.05.042 | Study of the level of alanine transaminase (ALT) in the blood | 190 | 1 | 190 |
| A09.05.041 | Study of the level of aspartate transaminase (AST) in the blood | 190 | 1 | 190 |
| A09.05.022.003 | Study of the level of total, free and bound bilirubin in the blood | 380 | 1 | 380 |
| A09.05.020 | Blood creatinine level test | 190 | 1 | 190 |
| A09.05.017 | Blood urea level test | 190 | 1 | 190 |
| A09.05.023 | Blood glucose test | 220 | 1 | 220 |
| A05.10.006.1 | Registration, interpretation, description and interpretation of electrocardiographic data (ECG) | 1 000 | 1 | 1000 |
| B03.016.006 | General (clinical) urine analysis | 285 | 1 | 285 |
| TOTAL: | 37075 | |||
Entorhinal cortex
The entorhinal cortex (EC) is a region of the brain located in the medial temporal lobe and functions as a hub in a broad network of memory and navigation. The EC is the main interface between the hippocampus and neocortex. The entorhinal cortex-hippocampus system plays an important role in declarative (autobiographical/episodic/semantic) memory and spatial memory in particular, including memory formation, memory consolidation, and memory optimization for past events. The EC is also responsible for preprocessing (familiarization) of input signals in the reflex membrane response of classical trace conditioning, the coupling of impulses from the eye and ear occurs in the entorhinal cortex.
The entorhinal cortex is generally divided into medial and lateral regions, with three bands of distinct properties and connectivity running perpendicularly throughout the region. A distinctive feature of EC is the absence of cell bodies, which should contain layer IV.
The superficial layers—layers II and III—provide EC projections to the dentate gyrus and hippocampus. : Layer II projects predominantly to the dentate gyrus and hippocampal CA3 regions; layer III mainly refers to the CA1 region of the hippocampus and the subbiculum. These layers receive input from other cortical areas, especially the association, perinasal and parahippocampal cortices, as well as the prefrontal cortex. . Thus, the EC as a whole receives highly processed information from each sensory modality and also makes contributions related to ongoing cognitive processes, although it should be emphasized that within the EC this information remains at least partially separated. The deep layers, especially layer V, receive one of the three main outputs of the hippocampus and, in turn, interconnections from other cortical areas that project into the superficial EC.
Brodmann area 28 is called the “entorhinal area”, Brodmann area 34 is called the “dorsal entorhinal area”.
The entorhinal cortex is the first area of the brain to be affected by Alzheimer's disease; A recent study using functional magnetic resonance imaging localized the first lesion to the lateral entorhinal cortex. The volume of the left entorhinal cortex is inversely correlated with the level of alpha band phase synchronization between the right anterior cingulate and temporo-occipital regions. Aerobic exercise may have a positive effect on the medial temporal lobe memory system (which includes the entorhinal cortex) in healthy young adults.