The brain is the most complex organ of the human body; hundreds of scientific works are devoted to its structure and functioning.
The work of all organs without exception is controlled by the brain. Not a single action (conscious or unconscious) occurs without his participation.
To perform such a large amount of work, the brain must be a well-oiled machine, in which every part is in its place and performs a specific function.
In addition to the well-known cerebral hemispheres, the brain includes: the cerebellum, pituitary gland, hypothalamus, corpus callosum and medulla oblongata. Below we will talk about the corpus callosum and its place in the functioning of the nervous system.
What is the corpus callosum
The cerebral corpus callosum (CC), or commissure major as doctors call it, contains tens of millions of nerve endings.
It is a dense whitish substance covered with a thin layer of gray matter. MT, along with two other spikes, is a connecting link between the hemispheres of the human brain. It ensures interconnection and transfer of information between individual segments.
Anatomy of the corpus callosum
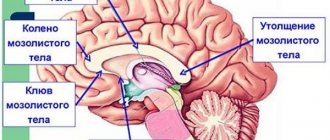
The commissure is oblong, 2–4 centimeters wide, its length depends on age and gender, but does not exceed 10 centimeters. Consists of several departments.
The splenium of the corpus callosum is a thickening in the posterior part. The middle section is the trunk. The main part is 2/3 of the entire length of the solder.
The front one is a knee that ends in a thin beak.
The structure of the MT is such that it lies deep in the longitudinal sulcus and connects only the hemispheres, without affecting the rest of the brain.
Functions of the organ
For a long time after its discovery, scientists could not understand what specific functions the corpus callosum performs. It was initially assumed that it contained a focus of epileptiform activity.
For patients with epilepsy, surgeons cut it open to eliminate seizures. The seizures passed, but people's behavior changed. Thus, a patient with a dissected corpus callosum hugged his wife with his right hand and pushed her away from him with his left.
And only experiments on animals, and subsequently with the participation of a volunteer, made it clear:
- The obvious function is to physically connect the right and left hemispheres, since the corpus callosum is located deep in the longitudinal fissure between the hemispheres. Nerve fibers connect both symmetrical and asymmetrical sections of different hemispheres, as well as different sections of the same hemisphere.
- Information communication between the hemispheres. Neuronal fibers (white matter) fan out in all directions, transmitting information received by different lobes of the hemispheres.
- Coordination of the hemispheres. MT ensures not only the exchange of received information between the left and right hemispheres, it is also responsible for analyzing this information and responding adequately.
Syndromes of lesions of the corpus callosum.
The corpus callosum unites the anterior (frontal), middle (temporal, parietal) and posterior (occipital) sections of the cerebral hemispheres and is accordingly divided into anterior, middle and posterior sections.
Since the 60s of the 20th century, after the operation of cutting commissures began to be used in a number of countries for the treatment of epilepsy. After such an operation
a whole complex of new, previously unknown symptoms arises, which have been designated as “split brain” syndrome. The reason is the deterioration or cessation of normal interaction between the cerebral hemispheres, which can be regarded as an independent factor (or factors).
Split brain syndrome is described as consisting of a range of symptoms. These symptoms vary at different stages of the postoperative condition.
1. At the first stage (immediately after surgery), patients experience severe memory impairment, sometimes confusion, but later these symptoms disappear (or significantly decrease and become almost invisible during general observation of patients) and others come to the fore. These include clearly defined disorders of coordination movements in which both limbs are involved (for example, typing, riding a bicycle, etc.). At the same time, these movements are not disturbed if the patient performs them with one hand.
2. speech symptoms: difficulties in naming objects presented in the left halves of the visual fields (when visual information enters the right hemisphere). Experiments have shown that patients recognize the objects shown (they can choose them from those shown in the pictures), but cannot name them. This symptom was called "anomia". Patients cannot read a word presented to the right hemisphere, although they seem to understand its general meaning, since they select the desired object (or objects of the same category).
3. A special group of symptoms consists of disorders called “discopy-dysgraphia”: patients with a “dissected brain” cannot write and draw with the right and left hands, as a healthy person does (although it is better with the dominant hand): with one hand they can only draw , and the other - only to write.
All these symptoms can be explained by a violation of the mechanisms of interaction of the cerebral hemispheres in the visual and motor systems. At the same time, this category of patients shows better recognition of objects by touch with the left hand than with the right. Unfortunately, a detailed neuropsychological analysis of patients with a completely “split brain” has not been carried out, and therefore a complete picture of this syndrome
unknown.
A study conducted on patients who underwent partial transection of the corpus callosum (due to surgery for an aneurysm in the anterior, middle or posterior sections) showed that three independent variants of the “split brain” syndrome associated with the site of transection can be distinguished. In this case, disturbances in interhemispheric interaction occurred only in one modality and their nature depended on the location of damage to the fibers of the corpus callosum.
Option 1: when cutting the anterior sections of the corpus callosum, disturbances in the interaction of the hemispheres manifested themselves mainly in the motor sphere;
Option 2: when cutting the middle sections, disturbances in interaction manifested themselves mainly in the tactile sphere;
Option 3: during transection of the posterior sections, disturbances in interaction manifested themselves mainly in the visual system.
A manifestation of a violation of interhemispheric interaction in the mid-posterior parts of the corpus callosum was tactile anomia in the form of a violation of the naming of objects when palpating them (with eyes closed) with the left hand. When visually perceiving the same objects and feeling them with the right hand, their naming was intact.
Violation of interhemispheric interaction in the tactile sphere was also expressed in the form of difficulties in transferring poses from one hand to another. At the same time, patients were better able to identify objects by touch with their left hand than with their right. Disturbances in the interaction of auditory systems were detected by dichotic listening and appeared in the form of a decrease in the productivity of reproducing speech stimuli from the left ear (compared to normal data), and sometimes a complete inability to reproduce words presented to the left ear. This symptom was observed with damage to the anterior, middle, and posterior parts of the corpus callosum (in right-handed people).
A disruption in the interaction of the visual systems of the left and right hemispheres in this category of patients was detected in the case of presentation of stimuli to the left half of the visual field using a tachistoscopic technique. It was shown that in conditions
clinical neuropsychological experiment, visual anomia manifests itself with a combination of damage to the posterior parts of the corpus callosum and the pathways transmitting visual information from the right halves of the retinas of both eyes (i.e., with right-sided homonymous hemianopsia). In these patients, due to loss of the right halves of the visual field and damage to the posterior parts of the corpus callosum, visual information does not enter the left hemisphere and verbal assessment of stimuli becomes impossible. When the posterior parts of the corpus callosum are damaged, patients also experience the phenomenon of “discopy-dysgraphia”: they can write only with the right hand, and draw only with the left, although before the operation they performed both tasks with both hands. This shows that the left (leading) hemisphere continues to control the right hand in these patients, but its control of the left is incomplete. The right hemisphere completely controls the movements of the left hand with limited control of the right
.
Corpus callosum in men and women
Scientists have not yet reached a unanimous opinion on the relationship between the size of the corpus callosum and the functions it performs. At first, American scientists argued that women have a wider MT than men, and this supposedly explains the peculiarities of women’s intuition.
A few years later, French scientists refuted this theory and stated that the male corpus callosum, in relation to the size of the brain, is larger than that of women, and the brain itself is larger.
But they were able to derive one pattern: the different density of neural fibers between the segments of the hemispheres responsible for speech is a distinctive feature of the weaker half of humanity.
In women, both hemispheres are involved in the work at once, while the brain of men uses one hemisphere to a greater extent than the other.
History of the study
Doctors performed the first operations on the corpus callosum to cure epilepsy. The connection between the hemispheres was disrupted, and the patients were actually cured of epileptic seizures. Over time, scientists began to notice some side effects in these patients - their abilities changed, behavioral reactions were disrupted. It was experimentally revealed that, after undergoing such an operation, a “right-handed person,” for example, could not draw with his right hand and write with his left. There were other deviations, for example between conscious behavior and unconscious reactions. One man who underwent such an operation said that he loved his wife, but at the same time he hugged her with his right hand and pushed her away with his left.
The corpus callosum was no longer dissected to cure epilepsy. A whole layer of activity has opened up for scientists to study the functions of each hemisphere of the brain. In recent decades, sexual dimorphism (differences) in the size of the corpus callosum in men and women, as well as in people in general, has been actively discussed. The dependence of its influence on differences in behavior and abilities is assumed.
Malformations of the corpus callosum and their consequences
The first trimester is the most important stage of pregnancy. It is during this period that all the main organs are formed, and it is at this time that they are most vulnerable. The neural tube forms towards the end of the trimester, at 12-13 weeks.
The expectant mother undergoes an ultrasound, and it shows whether the newborn has any abnormalities in the structure of the brain, including the corpus callosum, because they will lead to mental retardation.
Therefore, it is very important to monitor your health, undergo all examinations on time and take vitamin complexes during pregnancy.
The main malformations of the corpus callosum:
- Dysgenesis
- Agenesis
- Hypoplasia
All these defects entail a number of disturbances in the functioning of other organs.
But most importantly, they are the cause of mental retardation. Parents of children with these defects talk about fairly favorable prognoses if there are no concomitant diseases of the central nervous system.
Such children, of course, are doomed to take medications for life: nootropics that improve the nutrition of brain tissue, neuroleptics that correct behavior, hormonal and anticonvulsant drugs.
Such children are observed by neurologists and neurosurgeons. Rehabilitation is carried out by psychologists, defectologists, speech therapists, neuropsychologists, and psychiatrists.
The 30% chance of a favorable outcome that doctors give for such defects depends on the hard everyday work of the parents. It is necessary to deal with both physical and speech, psychomotor, and mental development.
The child will not always want to study. He can get tired quickly, become moody, absent-minded, even aggressive.
Agenesis
Agenesis of the corpus callosum in the fetus is the complete or partial absence of the main commissural commissure between the hemispheres.
It can be either an independent disease or part of other congenital defects, for example, Aicardi syndrome. Reasons for the absence of the corpus callosum:
- Genetic anomaly. A chromosomal mutation can be hereditary (not necessarily in the next generations, it is quite possible that the precedent was in the 5th-6th generation or earlier). An accurate diagnosis can be made by a geneticist after an examination.
- Intrauterine infection. Three decades ago, the term TORCH appeared, which unites the most common infections dangerous to the fetus - toxoplasmosis, mycoplasmosis, syphilis, rubella, cytomegalovirus and herpes. Unfortunately, they lead to serious developmental defects, miscarriage and death of newborns.
Partial agenesis of the corpus callosum is not so dangerous. The functions of the missing areas are taken over by the neighboring segments, as well as the anterior and posterior commissures. However, it also requires constant monitoring of the baby’s condition and drug treatment.
Usually the deviation is visible on ultrasound, but sometimes the disease goes unnoticed. In the first few months of life, the problem becomes obvious.
Symptoms of agenesis of the corpus callosum:
- Functions of vision and hearing are impaired. The baby hears poorly or does not perceive sounds at all, and does not focus his gaze on an object. This is noticeable already at 1.5-2 months.
- The size of the head, and therefore the brain, is smaller than normal. During a routine consultation, a neurologist measures the circumference of the child’s head with a centimeter.
- Disturbances in the structure of the bones of the facial part of the skull are especially pronounced in the area of the eyes and nose.
- Various forms of epilepsy - convulsions, freezing, loss of consciousness.
- Delayed mental, psychomotor and speech development.
Parents can notice these symptoms themselves and consult a doctor. There are several signs that can only be detected through examinations:
- tumors, neoplasms, cysts - both at the site of the corpus callosum and in other organs, most often in the stomach and intestines;
- adhesions and characteristic spots on the fundus;
- disturbances in the electroencephalogram can appear only during functional tests, although sometimes the EEG in such children represents a variant of the norm.
Hypoplasia and dysplasia
It represents disturbances in the development of tissues of both a separate area of the corpus callosum and the entire organ. It is caused by the same reasons as agenesis - chromosomal abnormalities, intrauterine infections and poor lifestyle of the expectant mother.
Smoking, drinking alcohol and drugs lead to improper formation of the fetal neural tube.
MT dysgenesis is not life-threatening, but problems are inevitable. First of all, such children have problems with oral and written speech, perception of light signals and reaction to external stimuli.
Hypoplasia of the corpus callosum of the brain is a general underdevelopment of the brain. Hypoplasia, like other developmental anomalies of the corpus callosum, can be an independent disease or be associated with other developmental defects.
Main features:
- disproportionate skull. As a rule, this is noticeable, but deviations can sometimes be insignificant;
- the structure of the convolutions is changed - they become flat;
- muscular dystonia. The baby's movements are uncertain, infants do not hold their heads well and do not lean on their arms. If the disease was overlooked in the first months of life, then at an older age awkwardness and clumsiness are noted. Children often fall and drop objects;
- disturbances in the functioning of the nervous system. Sometimes it is very difficult to predict the reaction of a sick baby to a particular stimulus;
- developmental delay. The baby begins to walk later than others and has difficulty mastering speech.
Usually, abnormalities in the structure of the brain are visible on ultrasound during pregnancy.
But poor quality equipment, low qualifications of the doctor, and the specific position of the fetus during the examination can make it difficult to make a diagnosis in the early stages. Up to two years of age, children with hypoplasia of the corpus callosum can develop on par with their peers, and only after this age do symptoms begin to appear.
There are several ways to define both hypoplasia and dysplasia:
- Magnetic resonance imaging - allows you to see organic lesions of the brain and all its parts.
- Electroencephalogram - shows how the patient reacts to certain stimuli and records epiactivity.
- Neurosonography - ultrasound of the brain through the fontanel. Possible only in the first 1.5 years, then the connective tissue is replaced by bone.
Intracerebral tumors of the cerebral hemispheres
Treatment of brain tumors, like all cancers, is complex and quite expensive. All activities carried out during the course of treatment can be divided into the following groups. Symptomatic therapy All measures belonging to this group do not affect the cause of the disease itself, but only soften its course, allowing to save the patient’s life or improve his quality of life. • Glucocorticosteroids (prednisolone) - relieve swelling of brain tissue and reduce cerebral symptoms. • Antiemetic drugs (metoclopramide) - relieve vomiting that occurs as a result of an increase in cerebral symptoms or after combined chemo-radiation therapy. • Sedatives - depending on the level of psychomotor agitation and the severity of mental disorders. • Nonsteroidal anti-inflammatory drugs (NSAIDs - for example, ketonal) - relieve pain. • Narcotic analgesics (morphine, omnopon) - relieve pain, psychomotor agitation, and vomiting of central origin.
Surgical treatment Surgical treatment of tumors of the brain and spinal cord is the main, most effective method, but removing a tumor from brain tissue is very difficult.
The indication for surgery is the diagnosis of a brain tumor itself. Refusal from surgery is determined only by taking into account contraindications. An absolute contraindication is, first of all, such a degree of severity of the patient’s general condition that any surgical intervention is unacceptable. In addition, a contraindication to intervention aimed at removing the tumor is localization in such parts of the brain as the brainstem, subcortical ganglia, and corpus callosum. With such localization of tumors, surgical interventions are possible, aimed only at reducing intracranial pressure. The general principle that most neurosurgeons currently adhere to is the rejection of palliative operations such as decompressive trepanations and the desire for maximum complete tumor removal, and for malignant tumors, especially glioblastomas, tumor removal is combined with resection of functionally insignificant parts of the brain adjacent to the tumor. Sometimes wide resection of the anterior or posterior parts of the hemisphere is combined with only partial removal of glioblastoma.
For malignant brain tumors, even of the widest extent, surgical intervention is an element of a complex of therapeutic measures. This complex includes radiation therapy, chemotherapy, or a combination of both. A feature of chemotherapy for brain tumors compared to chemotherapy for tumors of other organs is that for brain tumors not only drugs that penetrate the blood-tissue barrier can be used, but also those that do not penetrate it. They are injected into the tumor bed or into the cerebrospinal fluid system. A positive element of this method of administration is the absence of an inhibitory effect on hematopoiesis.
Radiation therapy Radiation therapy plays an important role in the treatment of brain tumors; its prevalence and great importance are associated with objective factors limiting surgical intervention. When planning radiation therapy for patients with brain tumors, it is very important to determine the rational amount of radiation. For this purpose, it is necessary to use data obtained during surgery, pre- and postoperative computed tomography, gamma encephalography, magnetic resonance imaging, angiography, pneumocystography, and radioisotope studies. Determining a rational level of radiation will avoid or minimize the negative consequences of therapy. The effect of radiation therapy is based on the effect of ionizing radiation on tissue cells located in the path of the radiation beam. External gamma therapy (DHT) is predominantly used to treat brain tumors. The optimal start time is 7-14 days after surgery. Irradiation is carried out locally to the area of the tumor or surgical intervention or completely to the entire brain if local irradiation is not possible. Gamma therapy is carried out in courses of 7-21 days, the total dose of ionizing radiation for total brain irradiation should not exceed 20 Gy, for local irradiation - 60 Gy. The size of a single radiation dose (per 1 session) ranges from 0.5 to 2 Gy. Radiation therapy is selected individually depending on the cellular composition of the tumor, its size and location. Despite its effectiveness, radiation therapy is a rather difficult procedure for the patient; its use is accompanied by radiation reactions. Depending on the types of tumors, different radiation therapy regimens are developed.
Chemotherapy Before chemotherapy, it is necessary to carry out histological verification of the tumor to select an adequate dose and the most effective drug. If surgery has not been performed, the diagnosis should be confirmed by stereotactic biopsy. Also, a prerequisite for chemotherapy is to determine the patient’s individual sensitivity to the drug. The route of administration is selected based on the possibility of creating the highest concentration of the drug in the tumor tissues. For chemotherapy, drugs of the alkylating group, antimetabolites, drugs of natural origin, antiblastic antibiotics, synthetic and semi-synthetic drugs are used. The most effective chemotherapy is combined with radiation therapy and a course consisting of several drugs.
The drugs are administered in courses lasting from 1 to 3 weeks, at intervals of 1-3 days, until the entire prescribed dose of the drug is administered. The drug is administered under the control of the blood picture, since all drugs used in therapy affect the most actively dividing cells, including bone marrow cells. Based on the results of the tests, the course of therapy may be interrupted, and in some cases even cancelled. Concomitant antiemetic therapy is also of great importance for the patient. An important parameter from the point of view of the patient’s quality of life is emetogenicity - the ability to induce vomiting. High emetogenicity indicates that 90% of those receiving the drug without antiemetic therapy experienced vomiting. According to this criterion, 4 groups are distinguished: • > 90% - high • 30-90% - average • 10-30% - low •
Adequacy of antiemetic therapy is achieved by a combination of drugs that inhibit the activity of the vomiting center, together with sedatives. The choice of a specific combination depends on individual sensitivity, duration of chemotherapy and financial capabilities.
The prognosis is favorable only after radical removal of angioreticulomas. For gliomas, it is unfavorable, differing only in the period of manifestation of continued growth and the life expectancy of patients after surgery. The more malignant the tumor, the shorter this period.