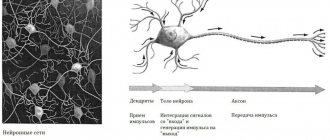
When the human brain works, only about 6% of its cells are used. The rest are in “standby” mode and if the “main team” is damaged or killed, they become active. However, atrophy disrupts this process, destroying both active and dormant cells.
Brain atrophy is the process of slow death of brain cells, reduction of its convolutions. The cortex takes on a flattened appearance, and the volume of the brain decreases. What is brain atrophy, what are its causes, types, main symptoms, treatment of the disease - the issues addressed in this article.
What is atrophy that occurs in the brain
Atrophic changes occurring in the brain look like a compensatory increase in the volume of cerebrospinal fluid against the background of a decrease in the proportion of neurons (brain parenchyma). The condition resembles hydrocephalus with the difference that it does not reflect a focal loss of tissue volume, but progressive pathological changes in them. It is expressed in the partial loss of physical and mental functions, provoked by local damage to a certain area of \u200b\u200bbrain tissue. There are 4 stages of the disease.
Grade 1 atrophy occurring in the brain is characterized by the absence of pronounced symptoms. A person may experience headaches, be depressed, emotionally unstable, become irritable and tearful. Copes with the usual tasks of professional activity and lives a full life. If treatment is not started, the mild initial form gradually develops into stage 2, when a person loses communication abilities and emotional connections with others.
Neurological symptoms are more pronounced - motor dysfunction, movement coordination disorder. Pathological processes lead to inevitable and irreversible dementia. The third degree is accompanied by death - necrosis of areas of gray and white matter from which the brain is built. The patient does not control behavior and often requires hospitalization and constant medical supervision. The picture of cerebral atrophy occurring in the brain in adults and elderly patients is illustrated by the following symptoms:
- incoherent, uninformed speech;
- loss of professional skills;
- loss of orientation within space and time period;
- loss of self-service skills.
The number of complaints about poor health decreases as the destructive processes of cortical atrophy increase. This is an alarming signal indicating a deterioration in the adequate perception of one’s own physical and mental state.
Carrying out a brain examination for the presence of atrophy
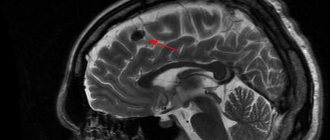
imaging of the brain during tomography Magnetic resonance imaging, using automated analysis of the results, allows us to identify even atrophies with minimal symptoms. At the initial stage, the pathology does not yet affect the patient’s behavior and well-being, so determining the presence of the disease is quite problematic.
Moderately expressed atrophic changes indicate progress in the development of the disease. The patient is prescribed therapy that can overcome the consequences of the disease.
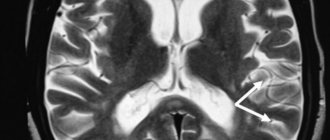
As a result of the study, it may be revealed:
- Disorders of the frontotemporal cortex are one of the most striking signs of developing Alzheimer's disease. As it develops, cells in the frontotemporal regions on both sides are destroyed, which leads to loss of reason and disturbances in the patient’s behavior. Subatrophies of the pole of the temporal lobe may also indicate a neurological disease of Pike.
- Moderate cortical cerebral atrophy - occurs in older people, most often in the age period of 50 years and older. Destruction of nervous tissue is observed throughout the brain. Subatrophy of the cerebral hemispheres is a symptom of senile dementia. Small lesions do not in any way affect the normal activity of a person and his mental abilities.
- Manifestations of diffuse cerebral atrophy - development is provoked by brain injuries. Although at the initial stage the disease manifests itself as a neurological disorder localized in the cerebellum, over time the disease spreads to the rest of the brain.
- Focal subatrophy is characteristic of patients suffering from epileptic seizures. Atrophic changes in the structurally immature brain substance lead to aggravation of the problem and development of the disease into the chronic stage. The cause of the disease can be injuries and pathologies that interfere with normal blood flow (osteochondrosis, cervical hernia, etc.). In this case, after eliminating the catalysts, the seizures go away on their own.
- Atrophy of the cerebral cortex with a decrease in the caliber of the cortical gyri. Disorders are associated with a hereditary factor and may indicate the development of Parkinson's disease, Alzheimer's disease, etc. An additional sign that people pay attention to is the presence of vascular insufficiency.
- Generalized cerebral atrophy - can be observed in a newborn baby as a result of fetal hypoxia or infection. A number of rehabilitation measures are carried out for the child.
- Subatrophy of the frontal parietal lobes usually begins as a consequence of injury or infection. Therapy is conservative. There is no specific treatment.
Types of pathology
The generalized form of cerebral atrophy involves multiple areas of nerve cells in the brain tissue. Diffuse brain atrophy is the uniform death of neurons in all areas of the brain structures. It develops as a result of arterial hypertension, which is characterized by damage to small vessels located in each part of the brain.
The initial symptoms of diffuse atrophy resemble dysfunction of the cerebellum. The progressive course leads to a rapid increase in symptoms, which makes it possible to differentiate the pathology at later stages. Unlike the cortical type, with diffuse atrophy the symptoms of damage to the controlling, dominant hemisphere are clearly expressed. With cortical subatrophy occurring in the brain, destruction and tissue destruction are only just beginning.
Subatrophy, which occurs in the brain, is a condition that precedes the stage of neuronal death. The mechanism of the disease has already been launched, destructive processes have begun, but the body independently compensates for the violations that have arisen. Subatrophic changes are accompanied by mild symptoms. Bihemispheric cortical atrophy occurs in the tissues of both hemispheres. Manifested by Alzheimer's syndrome.
Alcohol atrophy developing in the brain
Organic damage to the structures of the brain matter, which develops against the background of constant exposure to ethanol, is called toxic encephalopathy. Affects all parts of the brain. The cortical layers and cerebellum are especially sensitive to the negative effects of alcohol. Often leads to cranial nerve palsy. The frontal lobes are responsible for behavior, intelligence, emotions and moral qualities - properties that characterize a conscious personality.
Developing pathology causes atrophic changes in tissues and is one of the main causes of dementia. Dementia, as a consequence of alcoholism, is diagnosed in 10-30% of patients who abuse alcoholic beverages. A person becomes infantile and loses the ability for abstract logical thinking. As the disease progresses, the patient loses basic skills - the ability to brush teeth, tie shoelaces, and hold cutlery.
Multiple system atrophy
Covers multiple areas - the cerebellum, basal ganglia, spinal cord. If we understand in detail the topic of what atrophic degenerative changes are that affect the brain in a multisystem form, it is worth noting the progressive course, cerebellar ataxia (motor dysfunction) and autonomic failure syndrome. Manifested by loss of balance, tremors of the limbs, abnormal gait, erectile dysfunction. In the later stages, fainting, dizziness, parkinsonism, enuresis, and incoordination of movements are observed.
Cortical atrophy
Cortical atrophy is expressed by the death of neurons located in cortical structures in the frontal lobe. The frontal lobes are responsible for speech function, emotional behavior, determine personal characteristics, regulate human motor activity - planning and execution of voluntary movements. Cortical atrophy occurring in the brain negatively affects these abilities.
Atrophy of the cortex and frontal areas of the brain is predominantly associated with age-related destructive changes in tissues. Signs indicating cortical atrophy are behavioral disturbances and loss of intellectual abilities. With cerebral atrophy of the 1st degree cortical type, the patient is characterized by unmotivated actions that do not comply with generally accepted ethical standards.
A person cannot explain the reasons or assess the consequences of his actions. A characteristic sign that indicates atrophy affecting the frontal lobes of the cerebral hemispheres is regressive changes and personality degradation. Cognitive abilities decrease, the ability to think, remember, and concentrate is lost.
Atrophy affecting the cerebellum
The cerebellum is the department responsible for motor coordination. Destructive changes are manifested by malfunctions of the musculoskeletal system, imbalance, disorders of swallowing functions and eye control. The tone of the skeletal muscle corset decreases. It is difficult for a person to keep his head straight. Enuresis is often observed.
Causes
Cerebral atrophy of the brain most often becomes a consequence of pathological processes occurring in the human body. Moreover, the disease can be caused by several factors at once, aggravating the situation. Brain atrophy may occur as a result.
- Deviations at the genetic level
Atrophic changes occur against the background of the development of Pick's disease and Alzheimer's disease. Pick's disease is primarily characterized by damage to the frontal and temporal parts, which manifests itself in specific symptoms in the patient. These symptoms, combined with instrumental diagnostic methods, make it possible to quickly and accurately identify pathology.
The patient's thinking and memory deteriorate, and there is a decline in intellectual activity. The patient degrades as a person, becomes withdrawn, in communication one can notice predominantly the same type, simple phrases, repetition of the same thought is possible, speech takes on a primitive character.
Alzheimer's disease is characterized by a deterioration in the process of thinking and remembering; personal changes occur in the later stages of the pathological process.
- Cerebral atherosclerosis and hypertension
Atherosclerosis is fraught with the formation of plaques and clogging of blood vessels, which impedes blood flow and nutrition of cells. This pathology leads to oxygen starvation of brain neurons and subsequent death.
- Intoxication of brain cells
Obtained as a result of consuming alcoholic beverages and potent medications. With this effect, both the cerebral cortex and subcortical structures are affected. Brain cells have a low ability to regenerate, and with prolonged constant negative exposure, the pathological process worsens.
- Traumatic brain injuries
Injuries, including those resulting from neurosurgical interventions. Cortical atrophy may result from vascular compression. When a head injury occurs, vascular damage can also occur, which leaves brain cells without nutrition and they begin to die.
- Increased intracranial pressure
- Chronic anemia
With low levels of red blood cells or hemoglobin. This leads to disruption of the oxygen circulation process, so that a sufficient amount of oxygen does not reach the brain cells, and brain cells die.
Symptoms
Initial signs of atrophy affecting the tissues and structures of the brain usually appear in people over 45 years of age. Pathology is more often diagnosed in female patients. Characteristic symptoms:
- Changing personality type. Apathy, indifference, narrowing of interests.
- Psycho-emotional disorder. Mood swings, depression, increased irritability.
- Impaired memory function.
- Reducing vocabulary.
- Motor dysfunction, impaired coordination of movements and fine motor skills.
- Deterioration of mental activity.
- Decreased performance.
- Epileptic seizures.
The body's regenerative reactions weaken. Reflexes are depressed. Symptoms become brighter and more expressive. Atrophic changes are manifested by Parkinson's and Alzheimer's syndrome. The following signs indicate a specific affected area:
- Medulla. Deviations in the functioning of the respiratory, digestive, and cardiovascular systems. Defense reflexes are suppressed.
- Cerebellum. Weakness of skeletal muscles, malfunctions of the musculoskeletal system.
- Midbrain. Inhibited or absent reactions to external stimuli.
- Diencephalon. Pathological deviations in the functioning of the thermoregulation system, disruption of the hemostatic and metabolic systems.
- Frontal lobes. Secrecy, aggression, demonstrative behavior.
Signs such as impulsiveness, previously unusual rudeness, increased sexuality, decreased self-control, and apathy indicate malfunctions in the functioning of the main organ of the central nervous system.
Symptoms and diagnosis of brain atrophy
The complex of clinical signs that occur with cortical atrophy directly depends on the degree of damage to the cerebral cortex or its deep structures, as well as on the prevalence of the pathological process. Thus, moderately severe cortical atrophy, which in most cases is the reason for the patient’s initial visit to the doctor, manifests itself in the following form.
The initial stage of the disease is asymptomatic. The presence of any neurological symptoms at this time is usually associated with the presence of another organic or functional pathology of the nervous system. Subsequently, patients note the appearance of episodic headaches and dizziness.
Subsequently, there is a significant deterioration in the patient’s thinking abilities and analytical ability. The level of critical thinking and evaluation of one’s actions decreases. It is possible to change the characteristics of speech, handwriting, and habits.
As the disease progresses, fine motor skills of the fingers and coordination of movements worsen. Memory impairments are noted. The patient loses the ability to use even everyday items, such as a toothbrush or TV remote control. Patients often lose the ability to make independent decisions and begin to copy someone else's behavior.
Causes of the disease
Understanding the topic of what atrophy that occurs in the brain is, it should be noted that this is always a secondary diagnosis that develops against the background of long-term damaging effects on the central nervous system. Doctors name several reasons why brain cells die:
- Genetic predisposition. The most important factor.
- Intoxication of the body, repeated with high frequency, associated with the use of alcoholic beverages and drugs.
- Injuries to the skull and soft tissues inside the skull.
- Insufficient blood supply to tissues, cerebral ischemia.
- Chronic anemia – insufficient oxygen supply. The condition occurs as a result of low concentrations of hemoglobin protein and red blood cells in the blood, which deliver oxygen to the tissues.
- Infections that affect the nervous system - polio, meningitis, Kuru disease, leptospirosis, brain tissue abscess.
- Diseases of the cardiovascular system - ischemia of the heart muscle, heart failure, atherosclerotic vascular pathologies.
- Decortication due to coma.
- Intracranial pressure. It is often the cause of cerebellar atrophy in newborns.
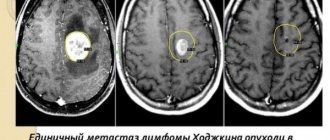
- Large tumors that compress surrounding tissues and interfere with normal blood supply to parts of the brain.
- Cerebrovascular disease is destructive changes in the vessels located in the brain.
If a person avoids mental activity, the risk of developing atrophic diseases occurring in the brain increases. Among the factors that increase the likelihood of the death of neurons located in the brain are smoking, low mental stress, chronic arterial hypertension, hydrocephalus, and long-term use of drugs that constrict blood vessels.
Causes of cortical atrophy development
The reasons for the development of age-related atrophic processes in the brain are complex. Thus, the following factors influence the formation of senile dementia:
- Impaired blood supply to brain tissue due to a significant decrease in vascular capacity (atherosclerosis)
- Deterioration of blood oxygen saturation, which contributes to chronic ischemic phenomena in the nervous tissue
- Activation of genetic factors of predisposition to atrophic phenomena
- Deterioration of the body's regenerative abilities
- Significant reduction in mental workload
It is important! In addition to all of the above, the chances of developing brain atrophy in old age depend to some extent on the level of mental development of the patient in his youth. It has been proven that people who have a high level of intelligence, speak foreign languages, and actively work intellectually are less susceptible to developing senile dementia.
Congenital cortical cerebral atrophy, in fact, is hypoplasia of the organ, since in this case its initial normal formation does not occur, in relation to which atrophy develops. However, in most cases this process is also called atrophic.
In some cases, atrophic phenomena can develop in adulthood. So, the factors in the formation of the disease in this case are:
Diagnostics
To determine after which cases of atrophied areas of brain tissue appear, diagnostic studies are prescribed. The difficulty of diagnosing in the early stages prevents correct, timely treatment and full restoration of functions. During the examination, the doctor determines the level of reflexes and reactivity - the ability to respond to external stimuli. Instrumental and hardware methods:
- MRI, CT. Allows you to identify cystic and tumor formations, hematomas, and local lesions.
- Ultrasound, neurosonography - in newborns.
- Dopplerography. Reveals the condition and patency of elements of the vascular system.
- Angiography is an X-ray examination of blood vessels.
Neurophysiological studies, including electroencephalography (determining the degree of brain activity), rheoencephalography (determining the state of cerebral circulation), diagnostic punctures, are carried out to identify the causes that led to damage to the cells that make up the brain tissue.
Symptoms
At the initial stage, the signs of the disease are smoothed out. Those closest to him begin to notice in the patient: lethargy, apathy, indifference to everything. It is possible to display previously unusual sexual activity, while denying moral boundaries. Further death of brain cells is manifested by:
- impoverishment of vocabulary, difficulties in choosing words to express emotions, describe an event, an object;
- rapid deterioration of intellectual abilities;
- loss of self-criticism;
- loss of self-control in actions and behavior;
- deterioration of motor skills.
The characteristic features depend on which area has undergone destructuring. Destruction of cortical tissues is characterized by:
- slow thinking;
- speech changes, timbre is distorted;
- the skills of memorizing information are lost;
- fine motor skills are lost.
The death of the medulla oblongata is manifested by:
- respiratory dysfunction;
- digestive problems;
- disorders in the functioning of the cardiovascular system;
- decreased immunity.
Damage to the cerebellum is accompanied by movement disorders: disturbances of balance, coordination, and muscle tone. Destruction of midbrain cells leads to loss of responses to external stimuli, intermediate - failure of the functions of thermoregulation and metabolism. All reflexes are lost when the anterior part of the GM undergoes destructuring.
When a large part of the neurons dies, the body loses its ability to maintain vital functions and death occurs. Necrotic changes in GM tissues are often caused by: chronic poisoning with toxins, TBI. The severity of the pathology depends on the location of the atrophy process and the stage of its development.
Instrumental methods are used to diagnose cerebral atrophy. CT allows you to identify areas of blood supply disturbance, vessels affected by a stroke, areas of hemorrhage, the presence of cysts, tumors in brain tissue. MRI makes it possible to evaluate pathological changes in all areas of the brain. Allows you to detect brain subatrophy - a precritical state, which significantly improves the prognosis of treatment. Allows you to identify the initial signs of pathology and a new diagnostic method - multislice tomography.
Treatment prescribed for brain atrophy
It is impossible to completely cure. Complex therapy is carried out with the aim of restoring the normal functioning of the nervous system, regulating metabolic processes occurring in the cells of the medulla, normalizing blood flow and blood supply to tissues. The disease is treated with conservative methods. Correct drug therapy inhibits the development of the disease. Taking into account the symptoms, the neurologist prescribes drugs from the following groups:
- Sedatives (calming agents).
- Tranquilizers.
- Antidepressants.
- Nootropic drugs that stimulate thinking abilities.
- Neuroprotectors that protect neurons from damage.
- Antihypertensive drugs and antiplatelet agents that lower blood pressure and improve blood counts.
The regimen is maintained simultaneously with drug therapy. The patient is advised to take walks in the fresh air, dosed physical activity, a healthy, balanced diet, activities related to mental activity to improve mental abilities, and memory training.
Therapy of atrophic pathology of the brain and prognosis of the disease
It is important! Age-related atrophy of the cerebral cortex cannot be completely cured. In this case, maintenance therapy is carried out aimed at slowing the development of symptoms of the disease. Atrophies acquired at a young age at their initial stage can be corrected provided the etiological factor is eliminated.
Drug treatment of atrophic brain pathology involves the use of the following groups of drugs:
- Drugs that improve brain metabolism and blood circulation in it (nootropic drugs). The most prominent representatives of this pharmacological group are: piracetam, Cerepro, Ceraxon, Cerebrolysin. Their administration leads to a significant improvement in the patient’s thinking abilities.
- Antioxidants (mexidol). They have a stimulating effect on regeneration processes, slow down atrophy, help increase metabolic rate, and counteract oxygen free radicals.
- Drugs that improve blood microcirculation. The most commonly prescribed drug is trental (pentoxifylline). The drug has a vasodilating effect, increases the lumen of capillaries, improves blood microcirculation and gas exchange through the vascular wall.
Some signs of cortical atrophy require symptomatic therapy. For headaches, patients are recommended to take non-steroidal anti-inflammatory drugs.
In addition to the use of medication, it is necessary to monitor the patient’s neuropsychic state. Moderate physical activity, daily walks in the fresh air, and self-care procedures are recommended. If the patient is in a neurasthenic state, the use of mild sedatives is indicated.
Cortical atrophy is a destructive process observed in the cerebral cortex. Most often, the disorder occurs in fairly old age, and it may also be associated with pathological changes occurring in the body.
Deviations inherent in this disease in most cases are located in the frontal lobes of the brain, which are responsible for thinking processes, and also thanks to them, control of behavior and planning is exercised.
In some cases, the process can affect other areas of the brain, but this is much less common. Typically, an extremely extensive process can lead to outright dementia. Manifestations of a focal nature do not have a pathological effect on the abilities of the brain.
The atrophy process is most dangerous for older people (over 50 years), since it is at this time that its slow progression occurs. The percentage of women susceptible to this problem is much higher than men. Ultimately, cortical atrophy leads to senile dementia.
Cases of cortical atrophy also occur in newly born babies, but this deviation is associated with severe heredity.
Prevention
Pathology is often a consequence of arterial hypertension and atherosclerosis. In order to prevent negative consequences, it is recommended to promptly treat diseases that provoke atrophic processes in the tissues of the brain matter. Doctors advise giving up bad habits, leading a healthy lifestyle, loading the brain with logical tasks, and stimulating intellectual activity.
Brain atrophy is a long-term pathological process that, in the absence of correct therapy, leads to dementia, disability, and complete dependence on staff. Often the patient requires hospitalization. In order to promptly identify and stop the development of the disease, at the first alarming symptoms it is better to consult a neurologist.
659
Degrees
Depending on the root cause and neglect of the disease, the following stages differ:
- The first stage of the disease does not manifest itself with obvious symptoms, is difficult to diagnose, often goes unnoticed and soon progresses to the second. Periodically, I have headaches and dizziness, which get worse over time. The development of pathology can be significantly slowed down if drug therapy is started in time and constantly adjusted.
- The second stage is manifested by obvious pathological changes in the structures of the brain. Analytical abilities decrease, cognitive impairments (speech, memory) appear, and fine motor skills are lost. Obvious behavioral changes occur: the manner of communicating, contacting people (the person becomes withdrawn, irritable, reacts violently to criticism, avoids communication);
- The third stage is characterized by: loss of self-control by the individual, neglect of the boundaries of cultural behavior. The person behaves strangely, unpredictably, and becomes unpleasant to others.
- At the fourth stage of the disease, the patient shows a lack of understanding of the people and events around him, withdraws into “his own little world”, talks to himself about something, answers inappropriately, speech becomes primitive;
- At the last (fifth) stage, complete prostration occurs. All brain matter atrophies, nerve impulses disappear. Dementia sets in, the patient is not aware of himself or those around him and needs constant care and supervision.
Pick's disease
This is a systemic degenerative disease with onset in presenile age, leading to personality and adaptation disorders, and subsequently to total dementia, most often of the frontal and frontotemporal type.
Pick's disease accounts for 0.4 to 2% of all cases of dementia in old age. The prevalence of the disease in people over 60 years of age is about 0.1%. Women get sick slightly more often than men (in a ratio of 1.7:1). The disease begins between the ages of 50 and 70 years. The average duration of the disease is six years.
The disease usually begins gradually and progresses quite quickly. The initial stage of the disease is manifested primarily by personality changes. If the pole of the frontal lobe suffers, then apathy and spontaneity predominate. When the orbital cortex is damaged, a pseudoparalytic syndrome develops with euphoria, disinhibition and impaired abstract thinking; memory does not change significantly. When the temporal lobes are damaged, stereotypies of speech, behavior and movement come to the fore. Other variants of the onset of the disease are much less common: a) asthenia and asthenodepressive symptoms, b) aphasia phenomena, c) psychotic disorders with delusions of persecution, jealousy, harm, d) memory loss, due to which there is a similarity with Alzheimer's disease.
In the middle stage of the disease, against the background of disturbances in the most complex forms of mental activity (planning, forecasting, understanding the meaning of life situations, flexibility, criticality, creativity), focal cortical disorders are also detected. Speech impairments usually predominate. This is dynamic, amnestic or sensory aphasia. Echolalia and standing speech patterns are characteristic. Agraphia, alexia, acalculia, and apraxia are relatively less pronounced. There are attacks of muscle relaxation without complete loss of consciousness, amyostatic syndrome, extrapyramidal hyperkinesis, and rarely spastic hemiparesis. The appearance of epileptic seizures most likely indicates Alzheimer's disease. The initial state is similar in its manifestations to the symptoms of the terminal stage of Alzheimer's disease.
The etiology and pathogenesis of the disease have not been sufficiently studied. Treatment is similar to that for Alzheimer's disease. Relatively early-onset personality and behavioral disorders usually require hospitalization.
Huntington's chorea
This is a hereditary neurodegenerative disease in the middle and second half of life with a predominant lesion of the striatal system of the brain and less severe damage to other subcortical nuclei and the neocortex. The main manifestations of the disease are decreased intelligence, psychotic phenomena and choreic hyperkinesis.
Due to the fact that the latter sometimes does not develop even in the later stages, the process is also referred to as “Huntington’s disease”.
The prevalence of the disease reaches 4–8 people per 100 thousand population. Among patients in psychiatric hospitals it is 1%. The peak incidence rate occurs between 35 and 50 years of age. The disease lasts from 1 to 25 years.
In approximately half of the cases, the disease develops “due to a nervous defect” (Davidenkov, 1932) in the form of a personality disorder, mental underdevelopment and motor “moronism” (clumsiness, poor handwriting, etc.). The disease does not have a single development pattern. Choreic dementia is characterized by damage to the most complex forms of intellectual activity and uneven mental performance. Intellectual deficits are believed to be based on gross disturbances of attention and spasmodic loss of direction in the movement of thoughts. As intellectual impairments develop, they move closer to dementia.
Psychotic phenomena are recorded in 60% of patients. In Alzheimer's disease they occur in 43.5%, and in Pick's disease - in 11% of patients (Sternberg, 1967). In the early stages of Huntington's disease, predominantly psychogenic disorders are observed, including depression with apathy, hypochondria, or dysphoria. Paranoid psychoses with delusions of jealousy, persecution, and poisoning are relatively common. Later, paraphrenic states with delusions of grandeur, hallucinatory and hallucinatory-paranoid psychoses may develop. The most common hallucinations are tactile, visceral and fragmentary verbal. Choreic hyperkinesis is usually slow, low-amplitude, separated by large intervals; It is also typical that they include torsion and athetoid components and occur against a background of mild muscle hypotonia. Muscle strength decreases, eyelid ptosis and dysarthria occur.
There are abortive forms of Huntington's disease: a) neurological, with a predominance of akineto-hypertensive syndrome; usually begins early, b) with typical hyperkinesis and minimally expressed mental disorders, c) with minimal hyperkinetic and severe mental disorders, d) stationary forms, in which, despite extensive symptoms, the disease lasts for decades, so that patients die from intercurrent diseases. Most patients die in a state of mental insanity; in the terminal stage of the disease, hyperkinesis usually decreases or stops.
It has been established that predisposition to the disease is inherited in an autosomal dominant manner and usually leads to atrophy of the striatum, and to a lesser extent, the cortex. Men get sick more often. Huntington described the disease in two brothers. In 12 families descended from them, 100 cases of the disease were described.
When treating patients, drugs that block dopamine receptors (phenothiazine derivatives, butyrophenones) or reduce the content of dopamine in tissues (reserpine, methyldopa) are used. Psychotic disorders are an indication for the use of aminazine, tizercin, propazine or teralen, and other antipsychotics. The results of therapy are usually disappointing. The prognosis of the disease is generally unfavorable.
Classification
The division of the pathological process is carried out according to several criteria. The main and most common is the type of disorder.
Primary form
Develops against the background of genetic abnormalities and defects. It is relatively rare, but presents enormous difficulties from a therapeutic point of view.
Recovery is impossible in principle; all that remains is to reduce the intensity of the symptoms. In this case, the prognosis is always unfavorable; the patient plunges into a state of deep disability in a matter of years, then dies.
The trigger mechanism for the onset of cerebral atrophy is injury, past infections, and other negative factors.
Secondary form
Seen much more often. The intensity of symptoms, the path and nature of the course, and other points depend on the specific cause.
In some cases, it is possible to quite successfully stabilize the development of the pathological process, maintaining the patient in a normal state for many years.
Degrees of impairment
The second method of classification is fractional, based on the degree of involvement of brain structures in the disorder.
- Cortical atrophy. Characterized by local changes in nerve tissue. As a rule, atrophy of the cerebral cortex occurs, and most often at the level of the frontal lobes.
A person quickly falls into inadequacy, loses the ability for emotional and mental self-regulation and becomes a burden for relatives.
- Multisystem form. It's diffuse. Slightly less common. A characteristic feature is the development of a group of foci of atrophy. The process occurs due to genetic abnormalities, congenital factors, injuries, infections. Possible development after a stroke. The treatment does not have much effect.
- Generalized atrophy. An even more pronounced form of the “drying out” process. The entire brain is affected. Mostly begins against the background of current dementia. Senile and other types, including Alzheimer's disease.
Stages of development
Subdivision is also possible according to the stages of development of the disorder. Then they talk about staging the disorder. There are three phases in the development of the problem:
- First. Accompanied by minimal atrophic changes. The patient does not suspect anything yet. However, neurological disorders are already present. The first signs include: decreased quality and productivity of thinking, impaired memory, and behavior. The patient is still able to be aware of himself and control his own behavior.
- Second stage. Accompanied by much more pronounced deviations. They become noticeable at first glance. Problems with thinking and speech are typical. Forgetfulness develops.
The fact that the emotional component is preserved is paradoxical. If a person is upset about something, he will quickly forget about it, but the negative affect will remain. Behavior gradually deteriorates. The patient becomes not quite adequate, and eccentric antics are characteristic.
- The third stage is determined by the total degradation of personality. The functions of higher nervous activity are lost. The patient is no longer able to think or act. We depend on the people who look after him.
Does not speak, reacts poorly to all external stimuli. Doesn't show emotion. There can no longer be a way out of this state. For several years the person continues to function this way. But most often they die faster, from stagnation in the body and complications.
Classifications are used by specialists in different variations. The main task is to most accurately describe the pathological process.
Therapy, its quality and the likelihood of effective help depend on understanding the essence of the phenomenon.