Previously, Shy–Drager syndrome, striatonigral degeneration, and olivopontocerebellar atrophy were classified as three separate diseases. However, upon deeper study, it turned out that the manifestations of the clinical symptoms of these diseases are common, so they were combined under one designation - multisystem cerebral atrophy.
Brain atrophy is the result of a process during which nerve cells gradually die and neuronal connections are destroyed. During such a complex deviation, significant functional impairments occur in the cortex and subcortex of the brain.
It is important to know! Brain atrophy often develops in older people. However, in rare exceptions, this disorder is recorded in a newborn.
What atrophies does the brain undergo?
With this disease, cells of the cortex and subcortical substance “die,” myelin fibers become thinner, neurons and their endings (axons) die. Atrophy of the brain is a consequence of injury, intoxication and hypoxia.
If the degeneration process has already started, the disease is fatal. With cerebral brain damage, life expectancy is sharply reduced. It takes 5-7 years from the appearance of the first symptoms to death.
Multiple system atrophy is accompanied by degeneration of cells in the basal ganglia, autonomic centers and cerebellum. The defeat of these areas determines the picture of the disease. Such multisystem degeneration and atrophy of the brain substance gives the clinical picture of parkinsonism, impaired autonomic functions and an unsteady ataxic gait. All these symptoms are called “multiple system atrophy,” although previously there were three separate diseases.
The death of neurons is an irreversible process. Multiple system atrophy starts with the symptoms of parkinsonism. Striatronigral degeneration gives symptoms of muscle rigidity, tremor, and postural disturbances. Multiple system atrophy is mistaken for Parkinson's disease.
What is it: cortical atrophy of the brain? The “bark” has a complex structure and is responsible for higher nervous activity. Each part has its own function. Somewhere is stored professional memory, the ability to create music, talk and see. With brain atrophy, the functions of higher nervous activity are lost, depending on the location of the lesion.
Atrophy of the brain substance is divided into cortical and subcortical. With multisystem damage, the striatonigral pathway and autonomic centers are destroyed and cerebellar atrophy begins, which leads to the progression of parkinsonian symptoms and a decrease in life expectancy. MSA has no effective treatment or effective prevention.
Types of atrophies: alcoholic, multisystem, cortical
At autopsy in patients with alcoholism, atrophy of the brain substance is detected: the cortex and subcortical structures. The most sensitive area is the frontal lobe. They contain centers responsible for behavior, emotions, and intellect. Brain atrophy due to alcohol intake leads to the loss of these functions and the disintegration of personality.
Shy-Drager syndrome, olivopontocerebellar degeneration, and striatonigral degeneration were previously considered three separate entities. But now they are combined into one form of the disease, which is caused by MSA. Causes, treatment and prevention are unknown. This disease leads to the death of the patient after 5-7 years.
With cortical damage, the most severe form of the disease develops. Vision may be lost (damage to the occipital lobes), hearing (damage to the temporal cortex). The disease leads to disruption of higher nervous activity.
Memory and intelligence are lost, behavior is disrupted (damage to the frontal cortex). It ends with the disintegration of personality. Pathology with predominant damage to the cortex inevitably leads to death.
Diffuse, cerebellar and posterior cortical types of the disease
The diffuse type of the disease is characterized by diffuse, non-localized lesions. Atrophy of the brain substance can occur in several structures at once (cerebellum, brainstem, cortex, basal ganglia). There is no clear clinical picture for this disease. Diagnosis of the disease is difficult. Characteristic signs on MRI: decrease in cortical volume, dilatation of the ventricles, diffuse lesions of subcortical structures. More often develops during intoxication conditions.
Cerebellar disorders can occur separately from multisystem lesions. They appear against the background of a stroke, tumor and injury. Atrophy of the brain substance affects only the cerebellum. The patient exhibits coordination problems, the gait becomes unsteady, and the clarity of the movements of the arms and legs disappears. A characteristic symptom is movements like a drunkard.
Senile dementia with disorders in the occipito-parietal cortex is a type of Alzheimer's disease. The disease leads to vision problems. The disease begins with the appearance of illusions, visual hallucinations and leads to complete loss of vision.
Diagnostics
Diagnosis of multiple system atrophy is based on analysis of the clinical picture and data from neuroimaging techniques. In this case, a mandatory sign is the presence of autonomic failure, which is confirmed by special clinical tests and daily monitoring of blood pressure levels. A reliable and accessible laboratory diagnosis of this disease has not yet been developed.
MRI of the brain can reveal a number of characteristic signs:
- Changes in the intensity of the signal from the putamen and globus pallidus, atrophy of the putamen, the appearance of a hyperintense (in T2 mode) slit-like stripe along the outer edge of the putamen.
- Atrophy of the brainstem and cerebellar structures. Changes affect the vermis, the cerebral cortex, the middle cerebral peduncles, and the base of the pons.
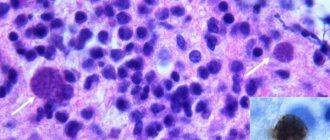
A definite (completely reliable) diagnosis is possible only with a pathomorphological post-mortem examination of the nervous tissue. Signs of the disease are dense glial cytoplasmic inclusions and degenerative changes in the olivopontocerebellar and nigrostriatal region.
MSA prevalence
Multiple system atrophy is a rare disease that is difficult to diagnose. Its prevalence in the world is 3-5 cases per 100,000 people.
In Russia, multisystem atrophy, in which there is multisystem degeneration (degeneration) of brain cells, occurs in 0.1 cases per 100,000 people. Such a low incidence leads to the idea of underdiagnosis of the disease “multiple system atrophy”.
MSA (multiple system atrophy) is a disease that is difficult to identify after the first visit to the doctor. Therefore, in Russia, a disease with slow death of brain cells begins to be treated quite late. In this case, multiple system atrophy is already in an advanced stage.
Forecast and preventive measures
At the present stage, MSA is considered an incurable pathological process. Symptomatic treatment can only alleviate the patient's condition, however, it is not able to stop degenerative phenomena.
The life expectancy of patients is no more than seven years. The fatal outcome is caused by complications of the bulbar symptom complex, intercurrent infection, and insufficiency of the cardiovasal system. Preventive measures have not yet been developed, because... There is no information about the etiofactor.
What is affected by MSA?
With multisystem atrophy of the brain, the following parts are affected: basal ganglia, cerebellum, brainstem. With Shy-Drager syndrome, brain neurons die in the area of the autonomic ganglia. Atrophy of the frontal lobes does not occur in MSA.
With Shy-Drager syndrome, the following symptoms appear: constipation, orthostatic hypotension, decreased function of the glands (sweat, lacrimal, salivary). Shy-Drager syndrome may resemble Parkinson's disease.
Degeneration with atrophy of the cerebral cortex and Shy-Drager syndrome do not lead to ataxia. It is caused by damage to the cerebellum. The patient's gait becomes unsteady, frequent falls occur, and coordination of movements of the arms and legs is impaired. Shy-Drager syndrome may precede ataxia or develop in parallel with it.
Brain atrophy: what is it? The slow death of neurons leads to the loss of certain functions. With diffuse cortical atrophy, hearing loss, vision loss, and auditory hallucinations begin.
Diffuse atrophy implies scattered lesions without clear localization. The brain is affected haphazardly, and it is very difficult to predict the consequences of the disease. Shy-Drager syndrome and MSA are characterized by a clearer clinical picture.
About the disease
Multiple system (multifocal, multisystem) atrophy is the extensive degeneration of glial cells in all structures of the brain (BM). The disease is abbreviated as MSA or MSA. Multiple system atrophy is a rapidly progressive, severe disease in which the spinal cord is often involved in the pathological process, leading to a decrease in the tissue of the central nervous system and disability.
Degeneration provokes the appearance of:
- dementia;
- shaking palsy - parkinsonism syndrome;
- dysfunction of the autonomic nervous system;
- cerebellar ataxia - a disorder of motor and speech function;
- insufficiency of the pyramids - the functioning of the central nervous system is disrupted.
Reference! MSA is a rare incurable pathology that occurs predominantly in men. The incidence is less than 6 cases per 100,000 population.
During the development of the disease, the subcortical nuclei (basal ganglia) inside the brain hemispheres are affected. They are located between the diencephalon and the frontal lobes. They consist of the striatum, gray and white matter, nigral (black) substance, and subthalamic nucleus. Histological examination of oligodendrogliocytes reveals accumulations of alpha-synuclein in cytoplasmic inclusions. This is unusual for the composition of neuroglial cells.
As a result of degeneration of the subcortical nuclei, the following is disrupted:
- coordination of movements;
- regulation of muscle tone;
- sensitivity of perception of visual, auditory and other stimuli;
- regulation of trophism, metabolism, respiration, urination, and other vegetative functions;
- development of reflexes, memory, other regulation of higher nervous activity.
MSA is more often detected in people over 50 years of age who have worked with harmful and toxic substances, pesticides, formaldehyde, and solvents. Patients with Parkinson's disease and Alzheimer's disease are at risk. The danger is that the pathology causes an irreversible process in the brain with the death of nerve cells. From the moment symptoms appear, life expectancy does not exceed 15 years. Death often occurs due to respiratory failure or sepsis.
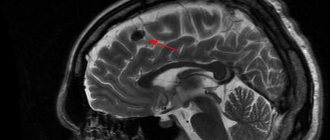
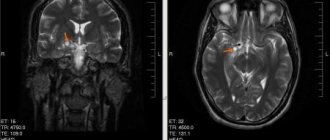
Figure 1. Imaging of the brain during tomography.
Until 2021, in ICD-10, multiple system atrophy was classified as code G90.3 under the name “multisystem degeneration.” Now in the directory there remains the parkinsonian type of MSA under the code G23.2 “MSA-P” and the cerebellar type – G23.3 “MSA-C”. In ICD-10-CM, pathology is numbered G90.3.
Causes and symptoms of the disease
The clinical picture of cerebral atrophy develops suddenly. Degenerative diseases are formed as a result of organic or toxic damage to neurons of the cortex and subcortex. The causes of the disease have not been established. The most likely risk factors may be:
- Head injuries;
- Tumor lesions;
- Intoxication;
- Chronic hypoxia;
- Vascular diseases.
How long do people with brain atrophy live? The severity of the disease depends on the number of neurons affected. The average life expectancy of a patient with MSA is about 5-7 years.
Atrophy of the frontal and temporal lobes (frontotemporal dementia)
Symptoms of atrophy may go undetected for several years. After the first clinical signs appear, doctors tend to think that the patient is developing Parkinson's disease. The main syndromes that predominate in the clinical picture:
- Parkinsonism;
- Ataxia;
- Autonomic dysfunction.
Signs of atrophy of the cells of the basal ganglia of the brain: trembling of the limbs, muscle tension, instability when walking. Slow steps, unsteady gait, uneven handwriting are symptoms characteristic of the patient.
Ataxia occurs when the cerebellum is damaged. At the same time, coordination of movements and the ability to move independently suffers. Autonomic dysfunction: constipation, indigestion, problems with urination and gland function.
Symptoms
The first sign of MSA is the onset of disease progression at an older age after 45 years. Symptoms develop quickly. Most people immediately develop parkinsonism and movement disorders. In 40% of cases, degeneration starts with autonomic dysfunction.
Changes in the initial stage are not always noticed by the patient. Among the first signs are pelvic disorders: erectile dysfunction, difficulty urinating or defecating, urinary/fecal incontinence. Every fifth patient begins to fall from the moment of progression of multiple system atrophy. The cause is considered to be orthostatic hypotension, muscle weakness, and cerebellar dysfunction.
Reference! The progression of MSA is characterized by the addition of other symptom complexes to the leading syndrome. That is, a person simultaneously exhibits autonomic failure in combination with signs of parkinsonism and cerebellar ataxia.
Differences in symptoms between different types of MSA
Primary symptoms depend on the class of multiple system atrophy. With the striatonigral type of MSA, signs of Parkinson's disease are immediately noticeable. Initially, the body responds to treatment with levodopa, then the effectiveness of the drugs is lost, and autonomic disorders worsen.
Primary signs of parkinsonian type of multiple system atrophy:
| Symptom | Explanation |
| Bradykinesia | All voluntary movements slow down. A person walks, speaks, writes, reads aloud more slowly. Coordination of movements and speech is preserved. A long conversation or the need to move causes rapid fatigue. |
| Rigidity | Stiffness of movement, tension in the muscles responsible for contraction and extension. The chin almost touches the clavicular area. In a horizontal position on the back, the head does not lie on the pillow, but this disappears after falling asleep. The limbs are bent at large joints, the torso is bent forward, the spine is stooped. During passive movement of the limb (performed by the doctor) under the fingers, the doctor feels the viscous resistance of the muscles. |
| Postural instability | A person cannot maintain balance. This is not associated with orthostatic hypotension, darkening of the eyes, or hypertension. |
| Tremor | The muscles of the torso, neck, arms, legs tremble during movement or rest. The tremor disappears when the patient performs the opposite action. That is, it stops or starts to move. |
With the olivopontocerebellar type of MSA, symptoms of cerebellar dysfunction are in the foreground. The patient begins to mince (step length decreases). There is unsteadiness of gait, muscle stiffness, deterioration in overall coordination of movements and fine motor skills. The tremor intensifies when approaching the target of the movement. It is difficult to change rapidly alternating actions.
With the cerebellar type of multisystem atrophy, dysarthria and oculomotor (oculomotor) dysfunction are manifested. Their symptoms:
- Muffled voice;
- Extended pronunciation of words;
- Chanted speech;
- Violation of sound modulation, phonation, breathing during pronunciation;
- Rhythmic involuntary movement of the eyeballs (nystagmus).
Shy-Drager syndrome in MSA is manifested by a disorder of the functions of the pelvic organs and glands. Fainting or collapse occurs due to a drop in pressure. Signs include impaired urination, bowel movements, decreased salivation, lacrimation, and sweating. Eye movements, conversation, and short-term cessation of breathing are observed during sleep. In men, erection deteriorates and impotence develops.
Reference! The progression of MSA is manifested by worsening symptoms of types 1–3 of multiple system atrophy. The clinic is supplemented by dementia, paralysis or paresis, inappropriate behavior, and complications of degeneration.
Etiology and pathogenesis
The etiology of multiple system atrophy is unknown. Scientists suggest that the death of brain neurons is associated with the accumulation of alpha-synuclein. This protein is deposited in the tissues of the brain and disrupts the conduction of nerve impulses. The reasons for the accumulation of the substance in multiple system atrophy are unknown.
What is brain atrophy? The cause of multiple system atrophy has not been established. There are suggestions about the genetic origin of the disease. Family cases of pathology were identified. The mutation was found on chromosome 19 as a marker of multiple system atrophy.
Pathogenesis of brain cell death in the elderly: molecules of alpha-synuclein and tau protein are deposited in glial cells. The accumulation of pathological substance in oligodendrogliocytes complicates interneuronal interaction. The pyramidal, extrapyramidal systems, motor cortex and cerebellum are affected.
The basal ganglia can also be affected when the brain atrophies. The shell is degenerating. Parkinsonism in multiple system atrophy manifests itself when these structures are damaged. The brain with MSA is atrophied in a certain localization. Such changes are visible only on PET.
Reasons for development
Scientists continue to study the causes, mechanism of development and triggering factors of MSA. There is no clear confirmation of a hereditary predisposition to the development of the disease. In a child, congenital atrophy of the brain occurs when a woman abuses medications, alcohol, or drugs during pregnancy.
During diagnosis, doctors identify possible causes of multisystem atrophy:
- Parkinson's or Alzheimer's disease;
- contact with neurotoxic substances;
- variability of the α-synuclein gene;
- alcohol and drug poisoning in people with addiction;
- brain and/or spinal cord injury;
- hypoxia of brain tissue.
Pathogenesis is difficult to study because the exact causes of multiple system atrophy are unknown. Studies have revealed the accumulation of tau protein in affected oligodendrogliocytes. This is detected in the cerebellum, pyramids, brain cortex, horns of the spinal cord in the thoracic and sacral regions of the ridge. At the same time, dopamine receptors and the substantia nigra are damaged, and α-synuclein accumulates in neuroglial cells.
Reference! MSA is characterized by an asymmetric decrease in white matter and impaired transmission of nerve impulses. Neurons suffer less than oligodendrogliocytes.
Clinical varieties and classification
Multiple system atrophy has several syndromes that develop simultaneously or follow each other. One of them may predominate in the clinical picture. MSA affects only adults; brain atrophy does not manifest itself in children. The following variants of the development of the disease are distinguished:
- Multiple system atrophy with a predominance of vegetative clinic (Shay-Drager syndrome);
- Multiple system atrophy with a predominance of parkinsonism (striatonigral atrophic lesions of the brain);
- Multiple system atrophy with cerebellar syndrome (olivopontocerebellar degeneration.
Multiple system atrophy in Shy-Drager syndrome is manifested by constipation, diarrhea, dysfunction of the genitourinary system, and dysfunction of the glands. The hallmark of Shy-Drager syndrome is orthostatic hypotension. When sick, the patient quickly “loses” pressure and often faints. Shy-Drager syndrome is treated with medications to increase blood pressure.
The Parkinsonian variant of multiple system atrophy differs significantly from Shy-Drager syndrome. With mild strianigral atrophy, the classic symptoms of Parkinson's disease appear: a slow shuffling gait, tremors, and muscle rigidity. The death of brain cells in this disease does not affect the white matter of the brain, and atrophy does not lead to dementia.
The third variant of multiple system atrophy is the ataxic clinical picture of the disease. It is characterized by damage to the cerebellum and brainstem. Diffuse brain atrophy is not observed. With multiple system atrophy, structures of only a certain localization are affected. OPCA is characterized by an unsteady gait, early falls, and lack of coordination.
So, the characteristic signs of multiple system atrophy:
- Brain atrophy is not typical in children; only people over 60 years of age suffer;
- The disease does not develop cortical atrophy (read what cortical atrophy is above);
- Atrophic changes in the brain do not occur diffusely. All foci are localized in subcortical structures;
- There is no critical cerebral vascular damage. The disease begins spontaneously and its cause has not been established.
Multiple system cerebral atrophy has an ICD 10 code of G90.3.
The disease is determined by a special clinical picture and MRI data (the study can be carried out at the medical center in Tushino, Aerodromnaya, 5). Reviews about the quality of the examination are the highest.
Classification
Doctors distinguish three forms of MSA depending on which syndrome is identified by the presenter. If this cannot be established, the patient is diagnosed with a mixed type of disease.
Classification of pathology:
| Leading symptom | Type of multiple system atrophy | Distinctive features |
| Parkinsonism | Striatonigral type of MSA | Slow movements, mask-like face, freezing in one position, “air cushion” symptom, tremors of the limbs, bent joints, decreased mobility. The striatum, the substantia nigra, is more susceptible to degeneration. |
| Autonomic failure | Shy-Drager syndrome | Dysfunction of glands and organs, pelvic disorders, hypotension, snoring, apnea. |
| Cerebellar ataxia | Olivopontocerebellar type of MSA | Poor balance, impaired fine motor skills, involuntary movement of the eyeballs, muscle weakness. The cerebellum, pons, and olives are more susceptible to degeneration. |
In the classifiers, doctors propose to remove Shy-Drager syndrome, since autonomic failure accompanies all forms of MSA. ICD-10 lists only the cerebellar and parkinsonian types of the disease.
Degrees of disease and diagnosis
With multiple system atrophy, a specific type 2 of the disease is distinguished (msa-p, msa-n). There are 3 degrees of severity. With a mild degree, symptoms are practically not expressed. Signs of tremor and unsteady gait may appear. The clinic is not enough to make a diagnosis.
At the average stage, the clinical picture of one of the syndromes predominates. Manifestations of the disease are clearly visible and significantly complicate the patient’s life. The doctor diagnoses, treats and registers the disability group. In severe cases, the patient is bedridden and requires constant care.
There are no characteristic MRI signs of brain atrophy in MSA. Doctors recommend using devices of at least 1.5 Tesla for diagnostics. However, in the initial stages, the pathology is difficult to distinguish from Parkinson’s disease. PET and SPECT provide more accurate localization of the lesion and the presence of foci of destruction of zones typical of MSA.
Diagnosis of multiple system atrophy is complex and impossible without other tests:
- Cardiovascular tests (orthostatic hypotension, low blood pressure and heart rate, bradycardia);
- Thermoregulation test;
- Electrophysiological study.
There are no characteristic specific signs of multiple system atrophy on MRI. Typical changes are determined: anomalies in the area of the basal ganglia, a “cross” in the area of the pons, degeneration of the pons and cerebellum.
Treatment
Multiple system atrophy has no specific treatment. It is difficult to stop or slow down progressive neurodegeneration. But doctors can help manage the symptoms of the disease. Several groups of drugs are used for this. Let's look at the treatment of MSA syndrome-by-syndrome.
Parkinsonism
Symptoms of parkinsonism are relieved with drugs that are used for Parkinson's disease (Levadopa). After a few years, the effectiveness of the products decreases. In this case, they are not indicated for the treatment of brain atrophy.
| Symptom | First line drugs | Alternative remedies |
| Bradykinesia, tremor, impaired postural stability, muscle rigidity. | Levadopa. When the patient tolerates the medication well, its dosage is increased to 1 gram per day. | If tolerance is poor, amantadines, dopamine receptor agonists, are used. |
Despite the high dosage of the drug, less than half of patients respond to Levadopa. Dopamine receptor agonists also produce a poor response. In addition, such prescriptions aggravate orthostatic hypotension and lead to hallucinations and dyskinesias.
The use of amantadines, especially in injection form, can have a positive effect with less severe effects of therapy. However, scientists recommend further research into the benefits of using this medication in patients with MSA.
Reducing the volume of fluid in the body
Multiple system atrophy with manifestations of orthostatic hypotension is corrected by diet, wearing an abdominal bandage and compression stockings. Treatment consists of an extended drinking regimen and salt intake. This allows you to maintain pressure and avoid fainting and falls.
Using a bed with a high headboard has also shown benefits in preventing low blood pressure during sleep and rest. Drug therapy has also been developed to relieve these dangerous conditions.
| Symptom | First line therapy | Alternative therapy |
| Orthostatic hypotension, fainting, dizziness. | Midodrine Droxidopa | Fludrocortisone Desmopressin |
Midodrine is an alpha adrenergic agonist. Its main properties are an increase in vascular tone and an increase in blood pressure. The tablets are taken orally. The initial therapeutic dose is 2.5 mg. It is increased to 5 mg 2-3 times a day. Side effects of midodrine include hypertension, increased lying pressure, bradycardia, heartburn, dry mouth, goose bumps, and problems with urination.
Droxidopa or L-DOPS. Trade name of the drug Northera. It is a precursor to norepinephrine. The main pharmacological properties are increased vascular tone and blood pressure. Recommended for use by the FDA. Unlike previous generation drugs, Droxidopa has fewer side effects and is well tolerated by patients. The most common negative manifestations of treatment are tachycardia, hypertension, headache with nausea and vomiting. They appear extremely rarely.
Fludrocortisone . A mineralocorticoid that can be used to treat fluid loss in the body. The main property is an increase in blood pressure. The drug is available in injection and tablet form. For low blood pressure, it is better to use oral medications. Side effects of fludrocortisone are typical of mineralocorticoids. These are increased pressure, peripheral edema, hypernatremia and hypocalcemia.
Desmopressin . The substance has an antidiuretic effect. Prevents excessive fluid excretion along with urine, maintains blood pressure. Intravenous, intramuscular and subcutaneous forms of administration are used.
Swallowing dysfunction
Some patients develop problems swallowing as the disease progresses. Liquid food mixtures and homogenized food help compensate for this condition.
If swallowing completely stops, it is necessary to install feeding tubes for nasal feeding or perform a gastrostomy. In this case, food is delivered directly to the stomach through a catheter. Parenteral feeding is possible, when nutrition is given intravenously.
Speech gymnastics is used to prevent swallowing dysfunction. Exercises allow you to mobilize the body's reserve capabilities and delay complications.
Urinary incontinence
As a result of disruption of the innervation of the pelvic nerves, patients develop urinary incontinence. Anticholinergic drugs are used to overcome the condition. Oxybutynin or tolteridine helps control bladder function.
Oxybutynin is an m-anticholinergic drug. It allows you to reduce voluntary and involuntary urge to urinate, and better control urinary function. The tablets are taken orally. There is a possibility of long-term use up to 2 years.
If, during conservative treatment of multiple system atrophy, acute urinary retention occurs, then catheterization is resorted to. To prevent disorders, gymnastics of the pelvic floor muscles, exercise therapy, and the use of biofeedback techniques are effective.
Biofeedback is the monitoring of physiological indicators and conscious control of them using special multimedia devices. The difficulty of treating incontinence is that performing special exercises is difficult due to the deep location of the muscles.
Many patients cannot contract them effectively, straining antagonistic muscles that increase intra-abdominal pressure. And the problem is only getting worse.
Classes with the biofeedback procedure involve the use of special rectal and vaginal sensors. They register the tone of the necessary muscles, stimulate them and allow a person to consciously contract them independently. Biofeedback procedures are carried out in a course of 15 days. They should be repeated 2-3 times a year.
Constipation
If you have problems with bowel movements, it is recommended to take dietary fiber. They enhance motor skills and stimulate peristalsis. In severe cases, laxatives (lactulose, senna tablets, macrogol) can be used.
Apnea
For frequent sleep apnea (short-term cessation of breathing), CPAP machines can be used. They allow artificial ventilation with constant positive pressure. The CPAP machine is a compressor. The air flow is continuously transmitted through the air duct into the patient's mask. Sleeping in a mask helps reduce morning fatigue, drowsiness, and heaviness in the head.
Impotence
To restore normal sexual function, it is permissible to use the drugs Sildenafil, Tadalfil. However, they should only be recommended if the patient is in good health. After all, they can lower blood pressure and cause weakness.
Dystonia
In rare cases, patients experience dystonia. Constant muscle spasm affects antagonistic groups. As a result, the patient develops uncomfortable and bizarre postures, which lead to loss of normal functioning and chronic pain in the affected muscles.
Botulinum toxin injections can be used to relieve this condition. The introduction of the substance relaxes the muscles and removes local soreness. The course of injections is about 7 procedures. The drug lasts for several months. After this, the injections must be repeated.
Sleep disorders and myoclonus
It is known that people with MSA develop REM sleep disorders. The patient behaves restlessly, may move his arms and legs, and perform other actions. This can lead to injury and disruption of night's rest. Therefore, a group of sedatives is used to help normalize sleep. Clonozepam, melatonin, and antidepressants are used.
Physiotherapy, rehabilitation and exercise therapy
Physiotherapy allows the patient to expand motor activity, get rid of spasms and muscle strain. For this purpose, magnetic laser therapy and electrical procedures (stimulation with low-frequency waves, wave interference) are used.
Therapeutic exercises and massage increase the patient’s activity and prevent the occurrence of contractures in the joints. Regular exercise improves the patient’s mood, prevents blood stagnation, and restores microcirculation.
Classes can be carried out both with preserved motor function and at the stage of bed rest. The course of exercises is developed by a specialist. The widespread use of technical rehabilitation equipment (wheelchairs, walkers, scooters) allows for long-term maintenance of socialization and everyday activity.
Multiple system atrophy has no cure. Patients are often offered quack therapy methods. For example, Makeenko T. “Treatment of disease with fly agarics.”
Remember, treatment with fly agarics has no scientific basis. Mushrooms are toxic; it is difficult to calculate the toxic dose for an elderly body. If Makeenko T. offers such a technique, one should doubt his professionalism.
Treatment
People with MSA are treated with symptomatic medications. They help eliminate the severity of parkinsonism, cerebellar ataxia and other signs of brain degeneration.
Symptomatic treatment of multiple system atrophy includes:
- levodopa medications;
- vasoactive agents;
- neurometabolic drugs;
- massage, water procedures, exercise therapy, other methods of physiotherapy;
- diet in compliance with salt intake;
- non-drug ways to eliminate orthostatic hypotension.
Parkinsonism in the initial stages of MSA progression is treated with combination drugs of levodopa with benserazide, carbidopa. It is replaced if it is poorly tolerated or ineffective with alternative therapy drugs. For atrophy of all types, dopamine receptor agonists and medications with the substance amantadine are used.
Manifestations of cerebellar ataxia are eliminated using physiotherapy methods. To alleviate the condition of MSA, medications containing clonazepam, gabapentin, buspirone, propranolol and other substances are prescribed.
For pelvic disorders against the background of atrophy, medications are used:
- Sildenafil (for erectile dysfunction);
- Macrogol, laxatives (in case of constipation);
- Alpha1-adrenergic receptor antagonist + cholinergic drug (urinary retention);
- Anticholinergic (involuntary or painful urination).
In case of bladder dysfunction, in addition to medications, periodic or continuous catheterization of the organ is indicated. Alternative medications include botulinum toxin injections. These injections are also prescribed for the treatment of respiratory disorders, captocormia, drooling, and dystonia due to MSA.
For orthostatic hypotension, it is recommended to sleep on beds with an elevated headboard and drink plenty of water rich in minerals. You must wear compression stockings. You can’t overeat or get up suddenly after waking up. It is recommended to learn isometric maneuvers. Mineralocorticoids and hypertensive drugs with midodrine are prescribed.
In case of breathing problems, ventilation or tracheostomy is indicated. Camptocormia is treated with physical therapy. Medicines with zopiclone or clonazepam eliminate sleep disorders due to MSA. For depression, a selective serotonin reuptake inhibitor (a group of antidepressants) is prescribed.
Reference! Clinicians continue to seek new treatments for multifocal atrophy. Etiological therapy cannot be used until the causes and mechanism of development of MSA are elucidated.
Clinical researches
Despite the fact that MSA is a poorly understood and deadly disease, scientists continue to study this neurodegeneration. In 1999, the European Society for the Study of ISA was founded. This is a consortium of researchers and scientific centers in Europe and Israel. He is involved in clinical trials and research to advance knowledge about severe neurological pathologies.
The main goal of EMSA-SG is to increase knowledge about the etiology and pathogenesis of the disease. The group uses the support of sponsors and implements developments to treat the symptoms of the disease. Information is exchanged with a research group from North America, China, and Japan.
Discoveries made in the field of studying neurodegenerative diseases:
- Alpha-synuclein, which was isolated from the brains of MSA patients, was an inducer of this protein in a healthy laboratory animal. In essence, he behaved like an infectious agent. A drug or process is currently being developed to help stop this spread;
- Scientists have linked the disease to mitochondrial damage. Thus, it has been demonstrated in models that the accumulation of alpha-synuclein and mitochondrial “breakage” lead the animal to the development of MSA;
- Markers and tests are being developed that will make it possible to quickly diagnose the disease, as well as monitor its course;
- Much attention is paid to creating a registry of patients with neurodegenerative diseases. Such research allows us to better understand the origin of MSA, inheritance, and the influence of natural, environmental and production factors;
- New drugs are being developed to treat the disease. A recent study showed the ineffectiveness of rifampicin for treating the symptoms of MSA.
The development of early biomarkers of neurodegenerative diseases is actively underway, and a common base of research work on this disease is being created. You can get acquainted with them by following the link.
Doctors
MSA treatment uses a multidisciplinary approach. A whole group of doctors cares for the patient. Specialists in movement disorders, cardiovascular system, urologists, gastroenterologists, somnologists, pulmonologists, ENT specialists, physiotherapists, occupational therapists, exercise therapy instructors.
Movement disorder specialists focus on problems affecting the nervous system due to diseases such as Parkinson's, MSA and others. In domestic medicine, the specialty of parkinsonologist (extrapyramidologist) is distinguished. This specialist has extensive knowledge regarding this type of disease and has experience working with and treating such patients. This is how he differs from a neurologist.
Orthostatic hypotension requires consultation with a cardiologist. He will help you choose a drug that will help you avoid weakness and fainting in an upright position. If there are problems with swallowing and speech, the patient should consult an ENT doctor. Classes with a speech therapist are also effective for initial problems with diction. He will suggest a course of exercises that need to be performed to support this area.
Problems with MSA affect almost every department. Only the joint work of highly specialized specialists guarantees quality care to the patient. However, most often the patient contacts a general practitioner. His knowledge and timely consultations with specialists allow the patient to quickly cope with new symptoms.
Treatment of multisystem cerebral atrophy in Russia is carried out in clinics in the neurology department and in private centers. Doctors treating multiple system atrophy in Moscow consult at the Federal State Budgetary Institution “Scientific Center of Neurology”. Registration is subject to a fee or by referral from a local health care institution.
Israeli clinics use innovative technologies for treating multisystem brain atrophy with mesenchymal thecal stem cells. Physiotherapists, speech therapists and sleep specialists also work with the patient. The use of stem cell treatment for multiple system brain atrophy is being tested.
End of life issues
Patients with MSA lose motor skills as a result of the disease. They require daily care. Need outside help to fulfill basic needs. Abroad, patients stipulate in advance what kind of assistance they require in the development of disability.
In our country, caring for a terminal patient, as a rule, falls on the shoulders of relatives. However, non-professionals cannot provide quality care for the patient. In addition, this regime causes “emotional burnout syndrome.” After all, most often caring for a sick family member does not relieve them from performing professional duties.
Other options for caring for a terminal patient:
- Hospices. Available subject to availability. There is the possibility of paid hospitalization. Among the disadvantages of the institution is the inability to control the quality of patient care;
- Professional nurses. 24-hour care requires high costs;
- Private nursing homes.
Complications
The consequences of MSA progression include urogenital infections, cystitis, urethritis, and kidney inflammation. Bacteria can enter the blood and cause sepsis. Against the background of respiratory disorders, pneumonia and sleep apnea often develop.
With multiple system atrophy, damage to the medulla oblongata is possible. This is complicated by a disorder of swallowing function and causes death due to paralysis of the respiratory center or asphyxia. As a result of degenerative processes, the functioning of the heart, vascular system, and cerebral circulation is also disrupted.
What should the patient's family do?
The disease progresses and the patient requires care. The first to appear are problems with swallowing liquid or solid food, independent movement and control of urination and defecation are impaired. Relatives of the patient may encounter the following problems:
- Registration of a disability group;
- Receiving social assistance;
- Finding patient care information.
You can assign the patient to a nursing home, where qualified staff will care for the patient. Boarding houses for people with this disease operate on a paid basis; a day’s stay costs from 1,500 rubles.
Link to a European support group for patients with MSA, as well as stories from the lives of patients in Russian and other languages.
Therapy for brain atrophy
There is currently no effective method of treating the disease. The process can be stopped only when the problem is secondary and there are ways to influence the root cause. It is impossible to restore dead tissue, so it is not possible to return the patient to a full life. If you do not deal with the problem, then as it progresses, somatic disorders will begin to appear, that is, internal organs will fail, which will inevitably lead to the death of the patient. Treatment of brain atrophy is symptomatic. It is possible to significantly influence the rate of degenerative processes only at the first stage of their formation. In such cases, giving up bad habits, normalizing the diet and an active lifestyle can significantly improve the future prognosis of the disease. In other cases, patients require constant care, and in the presence of somatic manifestations of the disease, hospitalization is necessary. Stabilization of the patient's condition is achieved using the following medications:
- Psychotropic drugs are prescribed to correct a person’s mental status. Many patients suffer from excessive irritability and mood swings during the process of nerve cell atrophy. Such changes are dangerous for the development of depression or, conversely, aggressiveness. To prevent this, means of varying action are used, depending on the clinical manifestations of the disorder.
- Drugs that stimulate cerebral circulation are actively used to slow down degenerative processes in nerve cells. They increase the intensity of nutrition and oxygen supply to tissues, which improves the condition of patients and prevents intensive neuronal death. This group of drugs includes drugs such as Cerebrolysin and Piracetam.
- Since the disease is often registered in older people, one of the main complications is arterial hypertension. It can also cause the development of insufficiency of brain functions. Appropriate means are used to correct high blood pressure. They can have a different mechanism of action: dilate blood vessels, correct cardiac activity, or remove excess fluid from the body. Often these drugs are used in combination, which allows for maximum effect.
In addition to pharmacological support for patients suffering from brain atrophy, constant proper care for them is also important. It can be carried out both at home and in medical institutions. It all depends on the severity of the disease. Doctors recommend that loved ones create a relaxed and friendly atmosphere at home, since positive emotions are important for correcting cognitive disorders. Patients suffering from the first stages of atrophy are advised to stop drinking alcohol and smoking, and normalize sleep and rest patterns. Adequate physical activity is also important. Even if it is difficult for a person to move, he needs to spend more time in the fresh air.
You can also fight the manifestations of brain atrophy with the help of folk recipes. Herbal teas using plants that have a calming effect have a positive effect. These include valerian, motherwort, mint and lemon balm. The use of infusions of viburnum and rose hips also has a beneficial effect, since the berries are rich in vitamins necessary to maintain immunity and correct metabolic disorders.
Prognosis and life expectancy
With atrophy, the cerebral cortex dies: how long does a person live? Nobody knows the answer to this question. From initial manifestations to death in MSA, an average of 3-7 years pass.
How long do sick people with brain death live? Modern resuscitation systems make it possible to prolong a person’s life even without a functioning central nervous system. Here the question arises about the advisability of such resuscitation.
The outcome of multisystem atrophy of the brain occurs when the respiratory muscles fail. The life expectancy of bedridden patients is reduced by respiratory infections and aspiration pneumonia. The consequences of the disease are very serious (after all, what is brain atrophy - disruption of all vital functions).
With cerebellar atrophy, death can occur as a result of injury. Life expectancy for this form of the disease ranges from 6-9 years (in the USA and Europe) to 20 years (according to Japan). It depends on the patient's genetics, conditions and care, environment and access to medical care.
How long can a person live with the death of the cerebral cortex? Doctors predict a lifespan of no more than 1-1.5 years.
What do you need to remember?
- With multiple system atrophy, irreversible degeneration of central nervous system tissue occurs in the brain.
- The causes of occurrence and the mechanism of development continue to be studied.
- In the ICD-10 reference book, two types of the disease were left: parkinsonian and cerebellar.
- In the MSA clinical picture, 2–3 syndromes are present simultaneously: autonomic failure in combination with cerebellar dysfunction and/or parkinsonism.
- During the diagnosis, the patient is tested for various types of central nervous system disorders and undergoes brain tomography.
- Treatment of multifocal brain atrophy involves the use of symptomatic therapy.
- Sepsis, bulbar palsy and other complications of MSA lead to death.
- There is no prognosis for recovery; the patient lives a maximum of 15 years.
- Prevention of MSA has not been developed because the causes of the disease are unclear.
Literature
- Shindryaeva N.H., Belova A.N., Levin O.S. Multiple system atrophy is common in Nizhny Novgorod. Collection of materials of the scientific and practical conference “Autonomic disorders in the clinic of nervous and internal diseases -2009” 2009
- Shindryaeva N.H., Levin O.S. Autonomic manifestations in patients with multiple system atrophy. Collection of materials of the III scientific and practical conference “Autonomic disorders in the clinic of nervous and internal diseases” 2010.
- Damulin I.V., Yakhno HH, Goncharov OA Comparative assessment of disorders of higher brain functions in various types of cerebral atrophy.// Journal. neurology and psychiatry S.S. Korsakov -1990.
- Ponomarev, V.V. Rare neurological syndromes and diseases. -SPb. Folio.
- Brown RG, Lacomblez L, Landwehrmeyer BG, Bak T, Uttner I, Dubois B, Agid Y, Ludolph A, Bensimon G, Payan C, Leigh NP; for the NNIPPS Study Group (August 2010). “Cognitive impairment in patients with multiple system atrophy and progressive supranuclear palsy.” Brain. 133 (Pt 8): 2382–93.
- Swan L, Dupont J (May 1999). “Multiple system atrophy.” Phys Ther. 79(5): 488–94. PMID 10331752.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th edition, (DSM IV). // Washington, DC: American Psychiatric Association, 1994.
- The Consensus Committee of the American Autonomic Society and the American Academy of Neurology (1996). “Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy.” Neurology. 46(5): 1470. PMID8628505.
Preventive measures
There is no effective prevention for MSA. The following measures are recommended to prevent degenerative brain diseases:
- Sufficient physical activity in old age;
- Constant training of intellectual potential (reading new books, learning languages);
- Control of somatic diseases (especially vascular), normalization of sugar levels;
- Refusal to work in hazardous industries or live in environmentally unfavorable areas.
MSA is a rare disease. Unfortunately, doctors cannot yet cure the disease or prevent its symptoms. However, it is possible to control the development of the disease and provide the patient with comfortable living conditions.
Degrees of atrophy
In the process of diagnosing the disease and determining the patient’s expected life expectancy, assessing the nature of the severity of degenerative changes plays an important role. The following classification is accepted:
- First degree atrophy is not expressed clinically. Rapid death of neurons occurs. This is due to the rare registration of the disease at this stage. The problem progresses, leading to the appearance of the first symptoms.
- The second degree is characterized by a change in the patient’s behavior and character. He becomes conflicted and irritable, often does not make contact with others. It is difficult for a person to maintain a conversation, he is constantly distracted and reacts inadequately to comments.
- The third stage is accompanied by a gradual loss of control by patients over their own behavior. They become unpredictable and even aggressive. The psycho-emotional state of such patients is unstable; these people can harm themselves and others.
- The fourth degree of atrophy leads to the patient's complete abstraction from reality. The victim is unable to understand what is being said and appears lost.
- The last stage consists of complete atrophy of both hemispheres of the brain. It is accompanied by serious cognitive and psycho-emotional disorders. Patients do not react in any way to external stimuli, and even if they are able to understand speech and current events, they do not experience any feelings or experiences about this.