A special place in the development of the individual and the human collective is occupied by the ability to transmit, receive and process sound signals. The ability to recognize and work with a complex sign system has made a person not just a highly developed organism, but a fully functional personality. Initially exchanging simple sounds, society eventually learned to convey complexly constructed verbal sentences. It is thanks to the presence of the temporal lobe that the implementation of the most complex mental function - speech - is possible.
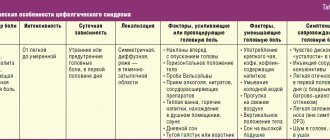
- Location
- Functions
- Fields
- Symptoms of the lesion
Anatomy
Its bundles begin on the inner side of the cartilage of the auricle (lat. pinna) between the anterior and superior ear muscles, its bundles fan out and attach to the tendon helmet (lat. galea aponeurotica) [2]. This muscle is a remnant of the ear muscles[4].
Innervation
The innervation of the temporoparietal muscle is carried out through the temporal branches of the facial nerve (lat. rr. temporales nervi facialis).
Blood supply
The blood supply to the temporoparietal muscle is provided by the superficial temporal and posterior auricular arteries (lat. aa. temporalis superficialis et auricularis posterior).
Diseases, injuries of the temporal region
Diseases
Among V.'s diseases. There are acute and chronic, inflammatory, including specific diseases, tumors of various tissues, fibrous osteitis. Of the acute inflammatory diseases of soft tissues, in addition to erysipelas, the edges usually spread from other parts of the scalp; the most common is deep phlegmon of V. o. Due to its anatomical features, pus accumulates in a closed space between the bone and fascia and hangs over the zygomatic arch, without a tendency to spread to the cranial vault. A breakthrough of pus into the infratemporal, pterygopalatine fossa and to the base of the skull is possible. The opening of the phlegmon is made by two incisions: the front one - slightly inclined anteriorly and the back one - vertical, opening the front and back parts of the fascial sac; if there is pus between the bone and the muscle, the latter must be carefully peeled away from the bone. A transverse incision should not be used, since this can cross vertically running vessels and nerves.
Osteomyelitis of the temporal bone is rare. More often it occurs as a result of the transition of the inflammatory process from soft tissues. Damage to the inner plate of the temporal bone is dangerous due to the possibility of pus breaking into the cranial cavity. There is a high probability of a purulent process transferring to the membranes of the brain in osteomyelitis after open fractures of the temporal bone. Treatment should be active - trepanation with removal of the affected bone, constant aspiration of pus (see Osteomyelitis).
Hron, specific inflammatory diseases (tuberculosis, syphilis) affect V. o. rarely.
Of the diseases of V. o. Non-inflammatory osteitis fibrous, fibromas, angiomas deserve attention. Fibrous osteitis of the Recklinghausen type (see Parathyroid osteodystrophy) occurs in two forms - generalized with multiple lesions of the skeletal bones and limited, in which only the bones of the skull are affected. The disease is rare. Fibrous osteitis of the skull is most often localized in the temporal bone, moving from there to the parietal and zygomatic bones. In V. o. a uniform swelling of bone consistency appears. The bone is sharply changed, thickened, turned into a spongy mass, external and internal plasticity are indistinguishable. This bone structure gives a characteristic x-ray picture with a mesh cellular pattern. The disease must be differentiated from sarcoma, which is characterized by faster growth. With a limited form of fibrous osteitis, surgical removal of the affected area of bone with plastic replacement of the defect can give a favorable result. With extensive lesions, the prognosis is unfavorable.
Rice. 2. Hanging fibroma of the temporoparietal region.
In V. o. Hanging fibroma (fibroma pendula) is relatively common. Fibromas are localized in the thickness of the skin or grow under its surface in the form of warty soft formations (Fig. 2). Treatment boils down to removing individual tumors within healthy tissue.
Of the angiomas of the integument of the skull, cavernous angiomas, which grow in the V. of the lake, are of greatest practical importance. not only the skin, but also the subcutaneous tissue, temporal muscle and can spread to the bone. In the latter case, the angioma communicates with the vessels of the cranial cavity and the venous sinuses of the dura mater. Angiomas are easily traumatized, resulting in bleeding, ulceration, and inflammation. The prognosis is often unfavorable. Treatment Ch. arr. surgical. Angiography helps to plan the upcoming operation (see). For small-sized cavernous angiomas, radiation treatment, injection of 96% alcohol into the angioma, and cryotherapy are used with good results (see Hemangioma).
Cirsoid arterial angioma is a vascular tumor consisting of dilated, tortuous nodular arterial trunks that directly extend into dilated venous collectors. It should be considered characteristic of the presence of pulsation and vascular noises: blowing - venous and systolic - arterial. These angiomas develop in the area of the branching of the temporal artery and other branches of the carotid artery and sometimes occupy almost half of the head. They cause pain of a neuralgic nature (damage to the auriculotemporalis) and constant pulsating noises that are very painful for patients. Treatment is surgical in combination with radiation therapy. The prognosis without surgery is unfavorable (risk of bleeding).
Rice. 3. Fracture (crack) of the scales of the temporal bone with transition to the parieto-occipital region. Rice. 4. Fracture (light oblique line at the top) of the pyramid of the temporal bone (x-ray, special placement).
Epilepsy of the occipital and parietal lobe
Any age of onset. Most patients with epilepsy of the occipital and parietal lobe were over 16 years of age at the onset of the disease. The disease rarely begins before age 6 years. This feature distinguishes TE from GE.
Seizures in TE are simple partial sensory attacks in the form of tingling, numbness, and an electrifying sensation. Paresthesias may be localized or distributed in a Jacksonian pattern. There may be a desire to move a part of the body or a sensation as if a part of the body has already moved. Most often, those areas that have the largest cortical area are affected - for example, the arm, shoulder and face. You may experience a numb sensation with a tingling tongue, a hard tongue, or a cold tongue. Sensory disturbances in the facial area can be bilateral. Sometimes, especially when the lower and lateral parietal lobes are affected, feelings of nausea, choking or suffocation appear. The sensation of pain occurs rarely and is more often perceived as a superficial burning sensation or an occasional, vague, very painful sensation.
Visual manifestations of damage to the parietal lobe can be colorful and take on an animal-like appearance. Metamorphopsia may occur with distortion, reduction or elongation of the image, which is more often observed with discharges in the non-dominant hemisphere. Along with these “positive” phenomena or productive symptoms, so-called negative phenomena are also formed, manifested, in addition to numbness, by a feeling of the absence of any part of the body, loss of the ability to recognize part or half of the body - asomatagnosia (more often with right-sided seizures). Severe dizziness may indicate involvement of the suprasylvian parietal lobe. Seizures of the left posterior lobe are accompanied by receptive and conductive speech disorders (Wernicke's center).
A fairly rare sensory disorder involving the paracentral lobule affects both lower extremities. Seizures of the paracentral lobule tend to be secondary to generalization.
In case of ZE, seizures are usually manifested by visual symptoms: simple - volatile visual porropsia (scotoma, hemianopsia, amaurosis, or sparks, flashes). More often they are in the visual field opposite to the place of discharge in the visual cortex. Illusions of perception with distortion of objects: one-sided diplopia, changes in size, distance, location of objects in a certain part of space, distortion of objects, sudden change in shape. Visual hallucinatory seizures can be complex and take the form of colorful scenes. Along with this, the scene may be distorted or reduced, and sometimes a person may see his own image (discharges in the temporo-occipital cortex).
Seizures may present without visual symptoms - contraversion of the eyes or head and eyes, twitching of the eyelids, forced closing of the eyes, a sensation of trembling of the eyes or the whole body, isolated dizziness or dizziness and unsteady walking, together with headache and migraine.
Neurology - focal neurological symptoms.
Assigned functions
The functionality of the temporal cortex is insignificant, however, it is highly specialized. The functions of the temporal lobe of the brain are associated with the perception, analysis and synthesis of speech, the perception of auditory information, and partly gustatory and olfactory information. Also, the location of one part of the seahorse determines another function - memory, namely its mechanical component. One area has a special purpose: Wernicke's center (sensory speech area) - located on the back of the superior temporal gyrus. This zone is responsible for the perception and comprehension of oral and written speech.
What matters is the functional asymmetry of the brain, that is, the location of the dominant areas of the cortex on the surface of the brain. This specificity of the central nervous system did not bypass the temporal lobe.
The left temporal lobe is responsible for the following functions (it should be noted that the list of tasks is based on the fact that the left hemisphere is dominant):
- Understanding audio information (music, words and speech);
- Short-term memory;
- Choice of words during a conversation;
- Synthesis of visual information with auditory information;
There is an interesting phenomenon here - synesthesia . Only 0.05% of the population has this phenomenon. The essence of the phenomenon is the ability to see the qualitative parameters of sounds in a different color spectrum. Physiologically, this is explained by the process of irradiation (spread of action potential), when the excitation of an overly irritated area of the cortex passes to the neighboring part of the brain. As a rule, famous musicians (Rimsky-Korsakov, Franz Liszt) possessed and still possess this ability. - The connection between music and emotions;
The right temporal lobe of the brain is responsible for the following functions and abilities:
- Recognition of facial expressions;
- Identification of speech intonation;
- Musical tones and rhythm;
- Memorizing and fixing visual data.
In addition to recognizing speech intonation, the non-dominant lobe also analyzes it and subsequently integrates images into the general emotional attitude towards the interlocutor. It is this part of the brain that allows a person to know whether his conversation partner is happy with him or wants to get rid of him as soon as possible.
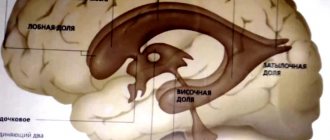
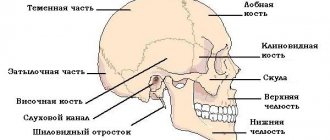
Location
The temporal lobe is part of the telencephalon and is included in the structure of the cortex. It is located on both hemispheres of the brain on the sides below, in close contact with neighboring areas - the frontal and parietal lobes. This area of the cortex has the most pronounced boundary lines. The upper part of the temple is slightly convex, and the lower part is concave. The temporal lobe is separated from all the others by a groove called the lateral (lateral). The close location of the temporal and frontal lobes is not accidental: speech develops in parallel with thinking (frontal cortex), and these two functions are closely interconnected, since the ability to formulate and express oneself clearly (speech) is ensured by the degree of development of mental functions.
The convolutions of the temporal lobe are located parallel to the grooves that limit the area. Anatomically, there are 3 gyri: superior, middle and inferior. However, the superior cerebral fold includes 3 more small convolutions located in the sulcus itself. This group of small structures is called Heschl's convolutions. The inferior gyrus of the temple borders the transverse medullary fissure. On the lower part of the temporal lobe, in addition to the inferior gyrus, additional structures are also distinguished: the hippocampal peduncles, the lateral occipitotemporal gyrus.
What fields are included?
Brodmann fields are territorial boundaries of the structural organization of different parts of the cerebral cortex. The area of the temporal lobe includes fields 42, 41 and 22. A lesion of field 42 entails a violation in the recognition of sounds. Auditory hallucinations indicate damage to the 22nd field, and with organic damage to the 41st field, full-fledged cortical deafness occurs (the same Wernicke's Aphasia).