Types of cranioplasty
Depending on what materials will replace the bone tissue, there are:
- cranioplasty with implantation of tissues of biological origin;
- plastic surgery of the defect using artificial materials.
If the patient’s own tissue is used during cranioplasty, then they speak of autoplasty. In the case of using biological preserved materials or tissues from animals, we are talking about alloplasty or xenoplasty.
Artificially created synthetic materials for cranioplasty are called explants. They can be made of metals (gold, platinum, steel, titanium, etc.) or acrylic resins (plexiglass, ethacryl, polakos K and R).
The list of synthetic materials used as implants on the skull is quite wide. They are considered inert, safe and quite durable, but are not without certain disadvantages, since they have both mechanical and biological effects on the human tissues surrounding them.
comparison of some types of transplant materials
Based on the time period from the moment of injury to the plastic surgery of skull defects, they are distinguished:
- primary cranioplasty - performed within the first two days from the moment of injury as the final stage of primary wound treatment;
- primary-delayed - carried out in the first 2 days - 2 weeks after the initial treatment of the wound, the tissues can be fused with loose connective tissue;
- early - no later than two months after the injury, during this period pronounced adhesions can be observed;
- late - after 2 or more months after receiving skull damage.
Autoplasty using one's own tissue can be free, when the tissue for transplantation is taken from a neighboring area of the head or another part of the body altogether. The disadvantage of the method can be considered the lack of nutrition in the transplanted tissue, which is why it may not take root. In other cases, autoplasty is performed with grafts on a feeding pedicle, which take root faster than a free tissue fragment due to preserved trophism through connection with the donor tissue. The disadvantage of the second method of cranioplasty is the impossibility of its use for large defects and the need for a repeat operation to separate the already established flap from the feeding pedicle.
Alloplasty, when the surgeon uses foreign materials, is much more widespread than autotransplantation. The source of material for skull plastic surgery can be bone, the dura mater of the brain, taken from a donor, specially processed and preserved.
When choosing a cranioplasty method, the surgeon is based on the parameters of the defect (diameter, nature of the edges, adequacy of treatment for wounds), the patient’s condition, the characteristics of the skin at the site of the proposed plastic surgery, the presence or absence of protrusion of brain tissue into the through defect of the skull, and the technical capabilities of the clinic.
If the patient’s condition allows, surgeons try to resort to bone-sparing cranioplasty operations for skull fractures. The necessary conditions for such operations are the satisfactory condition of the patient, the preservation of all vital functions, the absence of brain edema and protrusion of its tissue into the resulting bone defect.
To firmly connect bone fragments of any shape and size to each other, the method of adhesive osteosynthesis is widely used. Large fragments of the bones of the calvarium are preserved, while small fragments separated from the periosteum are first removed and treated with antibiotics, and then adhesive osteosynthesis is performed.
For injuries to the skull bones with the formation of free-lying bone fragments, surgeons can use the grinding technique, when bone fragments are turned into shavings placed on the dura mater of the brain, a film of fibrin, a thin sheet of gold, etc. The shavings of the patient’s own bone can be mixed with blood and special polymer. The grinding method is classified as a bone-preserving operation, since islands of bone chips subsequently serve as a source of new bone tissue formation.
Diagnostics
Since the replacement of the skull bones was caused by a head injury, regular brain examinations are necessary. The following methods are used for this:
- Magnetic resonance imaging.
- CT.
- Electroencephalogram to test cortical functions.
- Echo-EG.
- Rheoencephalography.
- Examination by a neurologist.
Important! The question arises: is it possible to do an MRI after cranioplasty using titanium plates? Yes, the procedure is allowed, since this material is not magnetic, unlike iron-containing objects.
Materials for cranioplasty and requirements for them
modern implants made by 3D printing
Regardless of the composition and method of obtaining a graft for cranioplasty, it must meet certain requirements:
- safety, low risk of infectious complications and other negative effects on the body (biocompatibility);
- absence of carcinogenic effect of artificial materials;
- high strength, low electrical and thermal conductivity;
- high survival rate;
- lack of tendency of the graft to stimulate a strong scar process;
- the possibility of using diagnostic techniques (MRI, etc.) after cranioplasty with artificial materials;
- ease of modeling and processing;
- convenience and completeness of sterilization;
- availability and reasonable price for most clinics.
Biological transplants obtained from the patient or donor are most often frozen or lyophilized (freezing under vacuum conditions). In this state, they can be preserved for a long time without losing their structure or changing their composition, which is extremely important for good engraftment in the future. In addition, lyophilized grafts are non-toxic and can be used for large cranial bone defects.
In cases where cranioplasty is performed on an emergency or urgent basis, frozen biological tissues may not be available, so surgeons use compositions based on acrylic resin (styracryl, butacryl, etc.). They are considered low-toxic, easily modeled and accessible, and provide hermetic closure of the bone defect. As the acrylic resin graft heals, it grows with connective tissue, which will firmly hold it in place after the adhesive composition has dissolved.
Experts in the field of neurosurgery are unanimous in their opinion that the best material for cranioplasty is the patient’s own tissue, so bone fragments are, if possible, completely preserved when treating a head wound. Bone fragments from the patient’s skull can be preserved in advance so that they can be used for skull surgery a little later. The disadvantages of the method are the resorption of bone grafts and a high risk of infection.
The most widely used grafts in modern neurosurgery are synthetic materials - metal plates, polymers, ceramics, etc. Among metals, preference is given to titanium, which is not only strong and lightweight, but is also well compatible with human tissue and has a minimal risk of infection. Among the polymers, polymethyl methacrylate, hydroxyapatite, and repirene are especially popular.
Today, neurosurgeons are increasingly resorting to the use of titanium grafts in the form of meshes, which are individually manufactured in accordance with the parameters of a particular patient’s defect. This approach allows you to reduce surgery time, reduce the risk of complications and provide maximum aesthetic results.
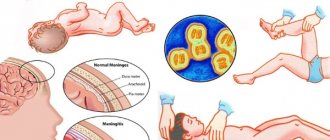
Often, with severe trauma to the skull, not only the bones of the head are damaged, but also the dura mater, which disrupts the tightness of the skull, creating the risk of infection, leakage of cerebrospinal fluid, damage to brain tissue and other dangerous complications. In this regard, it is extremely important to promptly and completely eliminate the defect of the dura mater.
One of the most effective ways to close a defect in the dura mater of the brain is the use of a donor membrane subjected to lyophilization. Such a flap can cover very large defects, is easily fixed to the edges of the wound defect, and prevents the leakage of cerebrospinal fluid. In an emergency operation, the surgeon can use polyethylene as a flap.
Restorative or aesthetic?
Previously, this operation was used only for medical reasons. However, today cranioplasty is in demand precisely as aesthetic surgery. A deformation on the skull resulting from an injury, an overly sloping forehead - all of this can be corrected by cranioplasty. However, restorative and aesthetic cranioplasty are different. Restorative cranioplasty often requires more serious surgery than aesthetic cranioplasty.
Today, cranioplasty is becoming much more accessible thanks to the use of the latest technologies. However, it still ranks almost first in its complexity. Therefore, if surgical intervention is required only for the sake of aesthetic correction, then you need to think carefully about whether it is worth undertaking all this.
If you do decide to undergo cranioplasty, then the most important thing to do is to choose a highly qualified surgeon. Only in this case will you be able to appreciate all the advantages of this difficult but necessary operation.
Indications and contraindications for cranioplasty
Indications for cranioplasty are:
- mechanical damage to the bones of the skull and dura mater, including penetrating, with splintered bone fractures, etc.;
- congenital malformations of the bone base of the skull;
- previous operations on the bones of the skull for wounds, tumors, malformations with the formation of a cosmetic defect.
In some cases, cranioplasty may be contraindicated. Thus, primary cranioplasty cannot be performed if:
- the patient’s serious condition, when there are breathing disorders, cardiac activity, coma;
- the presence of edema and swelling of the brain, its protrusion into the through defect of the skull;
- not removed foreign bodies in the cavity of the cranium;
- wound infection with the development of purulent inflammation;
- combined injuries of the skull bones and air sinuses.
Skull plastic surgery after trephination is performed to prevent the development of trepanation syndrome, in which the brain partially protrudes into the trepanation hole and is injured, which can cause pain, seizures and other neurological disorders. In addition, the removal of a burr hole has a cosmetic purpose.
In children, reconstructive and plastic surgery on the skull can be performed at a very early age due to congenital developmental anomalies or injuries to its bones. Timely treatment makes it possible to avoid disturbances in the growth and development of cranial bones and serious psychological problems during the adaptation of a child with an external defect to the children's team.
Any type of cranioplasty cannot be performed in the following cases:
- severe decompensated pathology of internal organs;
- blood clotting disorders;
- local inflammatory processes on the skull;
- general infectious diseases with fever;
- cerebral edema, coma.
Types of brain surgery
Craniotomy is a very complex neurosurgical operation involving the removal of a section of bone in a limited area of the skull. It is used to create surgical access for the removal of intracranial hematomas, various neoplasms, removal of damaged structures in case of skull injuries and as palliative treatment for increased intracranial pressure.
In order to minimize the risk of complications, the doctor collects anamnesis and selects the optimal intervention option. Contraindications for craniotomy are the following criteria: severe brain dysfunction, unstable condition of the patient, depression of consciousness with a score of less than 6 points on the Glasgow scale.
This could be titanium mesh, polyacrylates, bone cement, even plexiglass, which was used for cranioplasty in the 70s of the 20th century.
After the musculocutaneous flap with the aponeurosis is separated from the surface of the bone, it is turned down, fixed on napkins soaked in saline solution or hydrogen peroxide, and the surgeon proceeds to the next stage - the formation of the osteoperiosteal flap.
Preparation for surgery and postoperative period
Preparation for cranioplasty includes a standard list of examinations in the form of:
- general blood and urine analysis;
- biochemical blood test;
- blood clotting studies;
- tests for hepatitis, HIV infection;
- determination of blood group and Rh factor;
- electrocardiography, fluorography.
Cranioplasty surgery can take a long time and lasts on average 2-3 hours, so it is important to prepare the patient as well as possible. General anesthesia is used for pain relief. 2 weeks before the operation, anticoagulants are canceled, the day before the patient is given a cleansing enema, and in the evening food and water intake is stopped. The hair from the head in the intervention area is shaved off.
In the operating room, the surgeon treats the scalp with an antiseptic, makes an incision in the soft tissue and begins to restore the structure of the skull using prepared materials. After fixing the graft, coagulation or suturing of the bleeding vessels is performed, the soft tissues are stitched in the reverse order, and the sutures are treated with an antiseptic.
The course of the postoperative period is determined by the type of cranioplasty and the nature of the pathology. In the first days, the person undergoing surgery may be bothered by a headache and pain in the suture area, a feeling of a foreign body and discomfort in the head, so the attending physician prescribes analgesics and anti-inflammatory drugs. To prevent infectious complications, broad-spectrum antibiotics are indicated.
The consequences of cranioplasty depend on the nature of the pathology that led to the operation, as well as on the skill of the surgeon. The most common adverse effects are infectious complications, inflammatory changes in the wound area, bleeding, and excessive scarring in the area of graft placement.
Hospitalization in the absence of complications and a smooth course of the postoperative period lasts one and a half to two weeks. During this time, the tissues grow together, and on days 10-14 the sutures can be removed. Every day the wound is treated with an antiseptic and the bandage is changed.
examples of cranioplasty results
There are no significant restrictions in the lifestyle after cranioplasty, however, the person operated on should be careful when playing sports, the types of which are dangerous for injury are prohibited. Avoid possible injuries and head impacts, which could damage the implant or cause it to dislodge. Otherwise, the lifestyle after cranioplasty is the same as for all other people.
Consequences of installing titanium plates
Many people are interested in whether there are consequences of installing a titanium plate in the head. Patients who have undergone trepanation and plastic surgery may have:
- scars after injury, as well as surgeons’ scalpels;
- discomfort;
- inflammatory processes.
After surgical treatment, traces remain - white or purple scar tissue. Usually scars are clearly visible on the head, since hair does not grow in their place. This creates some aesthetic problems, especially for women. However, this can be corrected by using hair extensions or wearing wigs.
The consequences of a traumatic brain injury can also bother the patient after cranioplasty, because the plates replace bone, not brain tissue. After TBI, problems with speech and memory are often observed. Possible loss of practical skills and autonomic dysfunction. Medications are used to correct problems.
Sometimes the patient experiences discomfort caused by the presence of a foreign object in the body or the injury itself. In rare cases, the body reacts with an inflammatory reaction to the material, but titanium is very inert and has minimal immunogenic properties. Rejection occurs very rarely.