Scientists consider the frontal cortex as a set of formations that, from an early age, exhibit pronounced individuality in their anatomical structure. Among these formations there are those that are new, “ human ” fields that develop at a later age. These include field 46.
Field 46 is a “human field”, because it is an evolutionary neoplasm that differentiates late. Field 46 is the last to mature and reaches 630% of its original size. Because this field is inhibitory, you can notice that children do not control their movements and grab everything that is not lying well. This behavior is typical of monkeys.
General
It is impossible to specifically develop the frontal lobes of the brain in children. There is a misconception in society that physical activity promotes increased blood circulation in the brain, thereby developing all areas of the brain. Physical activity fills the motor centers of the brain, while the rest of the brain ' rests ', because When performing different tasks, the brain uses specific centers, rather than the entire brain.
Based on the above, in order to determine exercises for the development of the frontal lobes, we need to find out what functions the frontal lobes are responsible for, with which we can develop the frontal lobes.
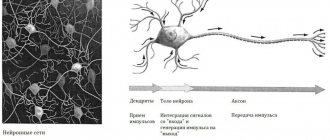
The frontal lobe, like the others, consists of white and gray matter.
Frontal lobe and its damage
Even though the frontal lobe is the largest lobe of the brain, it is often underestimated. routine neurological examinations. This is due in part to the attention to detail and rigorous testing requirements required to examine frontal lobe function. Since the solution of any cognitive task is associated with the function of the frontal lobe, but requires the involvement of several areas of the brain in the cognitive process both inside and outside the frontal lobe, some authors prefer to talk about systemic damage to the frontal lobe. In any case, frontal lobe dysfunction can lead to relatively specific clinical syndromes.
Traditional classification systems divide the frontal lobes into the precentral cortex (the region immediately anterior to the central or Sylvian fissure) and the prefrontal cortex, extending from the frontal poles to the precentral cortex, including the pars opercularis frontalis. The prefrontal cortex is divided into:
- orbitofrontal cortex (including orbitobasal or ventromedial and inferior medial areas);
- ventrolateral prefrontal cortex;
- dorsolateral prefrontal cortex,
- medial prefrontal cortex (containing the anterior dental gyrus, prelimbic and infralimbic cortex):
- caudal prefrontal cortex (which includes the frontal eye fields).
Each of these areas has broad connections both with other regions of the frontal lobe and with other brain structures.
The dorsolateral frontal cortex is responsible for planning, strategy, and executive functioning. Patients with dorsolateral frontal lesions tend to experience apathy, personality changes, abulia, and a lack of ability to plan or consistently carry out actions or tasks. These patients have poor working memory for verbal information (if the left hemisphere is primarily affected) or spatial information (if the right hemisphere is affected).
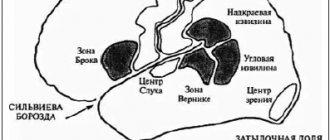
The frontal opercular part contains the speech expression center. Patients with left frontal opercular lesions demonstrate Broca's aphasia and difficulty finding words, whereas patients with exclusive right opercular lesions tend to develop expressive aprosodia.
The orbitofrontal cortex deals with response inhibition. Patients with orbitofrontal lesions typically demonstrate disinhibition, emotional lability, and memory impairment. Patients with such acquired sociopathy or psychopathic-like disorder are said to have an "orbital personality". Personality changes due to orbital damage include impulsivity, puerilism, crude humor, sexual inhibition, and complete disregard for other people.
Patients with lesions of the cingulate cortex usually exhibit akinetic mutism.
Patients with lesions of the inferior medial frontal lobe (basal forebrain) tend to exhibit anterograde and retrograde amnesia and confabulations.
Broca's aphasia, which developed as a result of damage to fields 44 and 45 in the left hemisphere, leads to a lack of fluency of speech, agrammatism, paraphasia, anomia and difficulty repeating words. Damage to the anterior, superior, and deep (but not superficial) part of Broca's area results in incorrect syntax and grammar, but the ability to repeat words and automatic speech is preserved. This disorder is known as “transcortical motor aphasia” (also called commissural dysphasia) and is also characterized by disinhibited echolalia. Memory impairment develops here only with extension of the lesion into the septal nucleus of the basal forebrain. Understanding of verbal humor is impaired in right-sided frontal polar pathology.
One of the seeming paradoxes of frontal lobe dysfunction is that doctors and psychologists may complain about the patient's “inability to do anything,” but, at least on superficial mental status testing, the patient appears normal or only mildly impaired. This dissociation may be a clue that frontal lobe dysfunction is present in the patient.
When the frontal lobe is damaged, attention is drawn to:
- Odd behavior: Does the patient say things he has never said before, such as “You're so fat” or “That dress is really ugly”?
- Patient's bad manners: Does the patient now take food with him and start eating in front of everyone else or drinking from other people's cups without asking?
- Lack of empathy in the patient and inability to understand the mental state of others: such dysfunction often leads to inappropriate behavior.
- Manifestations of apathy: Is the patient not taking care of family members and finances as he once did?
- Changes in the patient's sexuality or his judgment about possible sexual relationships.
Assigned functions
Evolutionarily, it so happened that the active development of the frontal lobes is not associated with mental and intellectual activity. The frontal lobes arose in humans through evolution. The more a person could share food within his community, the more likely the community could survive. In women, the frontal lobes arose for a specific purpose: sharing food. The men got this area as a gift. Without those assigned tasks that lie on the shoulders of women, men began to use the frontal lobes in a variety of ways (thinking, building, etc.) to demonstrate Dominance.
Essentially, the frontal lobes are inhibitory centers . Also, many people ask what the left or right frontal lobe of the brain is responsible for. The question is not posed correctly, because... in the left and right frontal lobes there are corresponding fields that are responsible for specific functions. Roughly speaking, the frontal lobes are responsible for:
- thinking
- coordination of movements
- conscious control of behavior
- memory and speech centers
- display of emotions
Parietal
In order to understand the functions of the parietal lobes, it is important to understand that the dominant and non-dominant side will do different jobs.
The dominant parietal lobe of the brain helps to understand the structure of the whole through its parts, their structure, order. Thanks to her, we know how to put individual parts into a whole. The ability to read is very indicative of this. To read a word, you need to put the letters together, and you need to create a phrase from the words. Manipulations with numbers are also carried out.
The parietal lobe helps to link individual movements into a complete action. When this function is disrupted, apraxia is observed. Patients cannot perform basic actions, for example, they are not able to get dressed. This happens with Alzheimer's disease. A person simply forgets how to make the necessary movements.
The dominant area helps you feel your body, distinguish between the right and left sides, and relate parts and the whole. This regulation is involved in spatial orientation.
The non-dominant side (in right-handed people it is the right side) combines information that comes from the occipital lobes and allows you to perceive the world around you in three-dimensional mode. If the non-dominant parietal lobe is disrupted, visual agnosia may occur, in which a person is unable to recognize objects, landscapes, or even faces.
The parietal lobes are involved in the perception of pain, cold, and heat. Their functioning also ensures orientation in space.
What fields are included?
Fields and subfields are responsible for specific functions that are generalized under the frontal lobes. Because The polymorphism of the brain is enormous; the combination of the sizes of different fields makes up a person’s individuality. Why do they say that over time a person changes. Throughout life, neurons die, and the remaining ones form new connections. This introduces an imbalance in the quantitative ratio of connections between different fields that are responsible for different functions.
Not only do different people have different margin sizes, but some people may not have these margins at all. Polymorphism was identified by Soviet researchers S.A. Sarkisov, I.N. Filimonov, Yu.G. Shevchenko. They showed that the individual ways in which the cerebral cortex is structured within one ethnic group are so great that no common features can be seen.
- Field 8 - located in the posterior parts of the middle and superior frontal gyri. Has a center for voluntary eye movements
- Area 9 - dorsolateral prefrontal cortex
- Area 10 - Anterior prefrontal cortex
- Area 11 - olfactory area
- Area 12 - control of the basal ganglia
- Field 32 - Receptor area of emotional experiences
- Area 44 - Broca's Center (processing information about the location of the body relative to other bodies)
- Field 45 - music and motor center
- Field 46 - motor analyzer of head and eye rotation
- Field 47 - nuclear zone of singing, speech motor component Subfield 47.1
- Subfield 47.2
- Subfield 47.3
- Subfield 47.4
- Subfield 47.5
Structural features
The most important part is located in front of both hemispheres and is a special formation of the cortex. It borders on the parietal lobe, separated from it by the central groove and from the right and left temporal lobes.
In modern humans, the frontal parts of the cortex are very developed and make up about a third of its total surface. Moreover, their mass reaches half the weight of the entire brain, and this indicates their high significance and importance.
They have special areas called the prefrontal cortex. They have direct connections with different parts of the human limbic system, which gives reason to consider them a part of it, a control department located in the brain.
All three lobes of the cerebral hemispheres (parietal, temporal and frontal) contain associative zones, that is, the main functional areas that, in fact, make a person who he is.
Structurally, the frontal lobes can be divided into the following zones:
- Premotor.
- Motor.
- Prefrontal dorsolateral.
- Prefrontal medial.
- Orbitofrontal.
The last three areas are combined into the prefrontal region, which is well developed in all higher primates and is especially large in humans. It is this part of the brain that is responsible for a person’s ability to learn and cognition, and forms the characteristics of his behavior and individuality.
Damage to this area as a result of disease, tumor formation or injury provokes the development of frontal lobe syndrome. With it, not only mental functions are disrupted, but also a person’s personality changes.
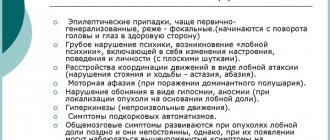
Symptoms of the lesion
Symptoms of the lesion are revealed in such a way that the selected functions are no longer adequately performed. The main thing is not to confuse some symptoms with laziness or imposed thoughts on this matter, although this is part of frontal lobe diseases.
- Uncontrollable grasping reflexes (Schuster reflex)
- Uncontrolled grasping reflexes when the skin of the hand is irritated at the base of the fingers (Yanishevsky-Bekhterev Reflex)
- Extension of the toes due to irritation of the skin of the foot (Hermann's sign)
- Maintaining an awkward arm position (Barre's sign)
- Constantly rubbing your nose (Duff's sign)
- Speech Impairment
- Loss of motivation
- Inability to concentrate
- Memory impairment
The following injuries and illnesses may cause these symptoms:
- Alzheimer's disease
- Frontotemporal dementia
- Traumatic brain injuries
- Strokes
- Oncological diseases
With such diseases and symptoms, a person may not be recognizable. A person may lose motivation, and his sense of defining personal boundaries becomes blurred. Impulsive behavior associated with the satisfaction of biological needs is possible. Because disruption of the frontal lobes (inhibitory) opens the boundaries to biological behavior controlled by the limbic system.
Treatment methods for LD injuries
Since there are many reasons for the development of frontal lobe syndrome, treatment is directly related to the elimination of the original disease or disorder. These causes may be the following diseases or conditions:
- Neoplasms.
- Damages of cerebral vessels.
- Alzheimer's disease.
- Pick's pathology.
- Gilles de la Tourette's syndrome.
- Frontotemporal dementia.
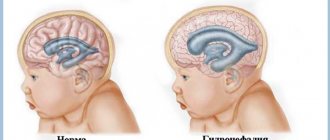
- Traumatic brain injury, including that received at birth, when the child’s head passed through the birth canal. Previously, such injuries often occurred when obstetric forceps were applied to the head.
- Some other diseases.
WE RECOMMEND SEEING: What percentage of a person’s brain actually works
With concussions and other skull injuries, the depth of damage to the frontal lobe is usually small, so the main symptoms often appear at the very beginning. With rest and appropriate treatment, they usually gradually disappear. In a tumor process with deep “germination” of the tumor, signs of ill health intensify over time.
Treatment of vascular disorders in the frontal lobes includes a whole range of medications that are selected individually for a particular patient. No two cases are the same, so there is no single treatment regimen. But the actions taken are approximately similar: the walls of blood vessels are strengthened, the blood is thinned, and cerebral circulation is improved.
In cases with tumors, whenever possible, surgery is used to remove the tumor; if this is not possible, then palliative treatment is used to maintain the vital functions of the body.
Specific diseases such as Alzheimer's disease do not yet have effective treatment and drugs that can cope with the disease, however, timely therapy can prolong a person's life as much as possible.